Birth Preparation After Trauma: A Trauma-Informed Roadmap for the Woman Who Has Never Found Things Easy

When I first got pregnant, I was young and naive, and I trusted that the systems that served us would also protect and keep me safe. By then, I had already had a diagnosis of depression and had begun to look into my past life experiences. I had seen that my past was shaping my present, but I did not have the full picture of how true this was. So when I found out I was pregnant with twins, the hospital made me take some preparation classes to care for the babies, which were provided by the hospital, mostly focused on caring for the twins in those first weeks and months. The focus was never really on the birth itself, or how it could happen, or what my options were. The message was clear: all that mattered was the healthy babies that would be cared for.
What I soon discovered is that there are no happy babies if there is a broken mother.
I ended up having a caesarean with the twins, and several complications that led to a complicated journey of recovery. This single event created ripples that led me to want to know why things happened the way they did, and how everything I had experienced, and the way I experienced the world, had shaped that event and my journey into motherhood.
Over my years working as a doula, I got to hear many versions of this story. It was the woman who had previous trauma and was concerned that, although she had worked through and healed that experience, she was not sure it would not show up in the birth room. Or the woman who had always felt just too sensitive for this world, who never quite felt she fitted in, and who was worried about what that meant for the birth. Or the woman with an ADHD or autism diagnosis who already knew that standard birth preparation did not work for her brain. Or the woman who was far from her family, still finding her footing in the social norms and cultural rules of the country where her baby was going to be born.
All these women came to me because they knew they had spent their lives adapting to schools, universities, jobs, pasts that had never quite fitted them. They suspected the same might apply to their birth.
The way I approached the preparation was never standard, but it was always rooted in awareness. An awareness they already carried, which was sometimes incomplete, sometimes just a quiet thought that they needed something different. And they followed that thread. They got curious.
If you recognise yourself in any part of these stories, this is for you. You were right to follow it.
Find your starting point
Each woman who finds her way here arrives through a different door. Select the one that feels closest to yours — or more than one, if that is truer.
You can select more than one.
Why Standard Birth Preparation Falls Short for the Women Who Find Their Way Here
These are different stories. But at some point, each of them was also mine. I have lived all of these versions, not as metaphor, but as lived experience, which I then had to make sense of, sit with, and eventually build something from.
That is why I know, with certainty, that standard advice was never going to be enough. Not for these women, and not for me.
Every time I walk alongside one of these women, the path is different. But the support is always rooted in the same four pillars I have built my practice on: person-centred care, trauma-informed practice, neuro-affirming support, and cultural sensitivity.
Those pillars are not a methodology. They are what I needed and could not find. And they are what I offer now.
How Past Trauma Can Shape Pregnancy, Labour, and Birth
Before we talk about what to do, it helps to understand why this matters, and why past trauma has more influence on the experience of giving birth than most maternity care acknowledges.
Trauma does not stay in the past. It lives in the body, in the nervous system, in the patterns of response that were learned during experiences that felt dangerous or out of control. When pregnancy begins, the body recognises something approaching: an intense physical experience, unfamiliar clinical environments, loss of control, exposure, and dependency on others. For a woman carrying perinatal trauma, a traumatic birth from a previous pregnancy, or trauma that predates pregnancy entirely, these conditions can activate a response that has nothing to do with the baby and everything to do with what the nervous system has already learned about safety.
Although many internalise it as mental health failing, It is in fact a body doing exactly what it learned to do. The difficulty is that a trauma response in the birth room, such as freezing, dissociating, losing language access, and feeling flooded with distress, can affect decisions, experiences, and the postnatal period in ways that persist long after the baby is born. Understanding this in advance is not catastrophising. It is in fact the most useful thing a woman with this history can bring into her preparation.
This roadmap was built for exactly that understanding.
Stage 1 — Recognition: What Is My Nervous System Carrying Into This Pregnancy?
Before a birth plan, before a sensory toolkit, before any practical preparation at all, there is one question worth sitting with honestly.
What am I actually bringing into this birth?
Not what you hope to bring. Not the version of yourself that will exist once you have done enough reading and preparation. What is already here, in the body, in the history, in the quiet worry that guided you to this page.
This is not a clinical assessment. It is an invitation to get curious, to follow the same curiosity that brought you here, about what your nervous system has already learned about the world, and what it is likely to do with the intensity of birth when it arrives.
Most women carrying any of the stories described above are perhaps holding more than one of them at once. The woman with a previous birth trauma is often also the one who has always felt things too deeply. The woman navigating a foreign healthcare system is often also the one who has healed something older and is quietly wondering whether it will hold. These categories are doorways, not diagnoses. You may have walked through more than one of them.
What recognition asks of you is not a decision. It asks only that you name, as honestly as you can, what is present, so that what comes next can actually meet it.
Some questions worth sitting with:
About your history. Is there a birth experience, your own or one you witnessed, that still lives in your body when you think about it? Is there something older than that, something that shaped how safe you learned to feel in your own body, in medical settings, in moments you could not control?
About your nervous system. Do you know how you respond when you feel overwhelmed or unsafe? Do you tend to fight for control, freeze and go quiet, disconnect from what is happening, or move toward the people around you? Your nervous system has a pattern. Birth will call it forward.
About your information needs. Do you feel safer the more you know, or does information sometimes spiral into anxiety? How do you make decisions under pressure? Who do you need beside you to think clearly?
About your support. Does the person who will be with you at the birth understand what you have carried into this pregnancy? Not the facts of it necessarily, but the weight of it? and do they know what you will need if something unexpected happens, and what you will not be able to ask for in the moment?
There are no right answers here. Recognition is not about concluding. It is about building the map before you need to use it, so that when the territory becomes unfamiliar, you are not navigating it for the first time.
What you find in this stage determines what Stage 2 looks like for you. For some women, the recognition stage surfaces something that needs processing before any planning can begin. For others, it confirms that the foundation is solid and the work ahead is primarily practical. Most women find something in between.
That is where the next stage begins.
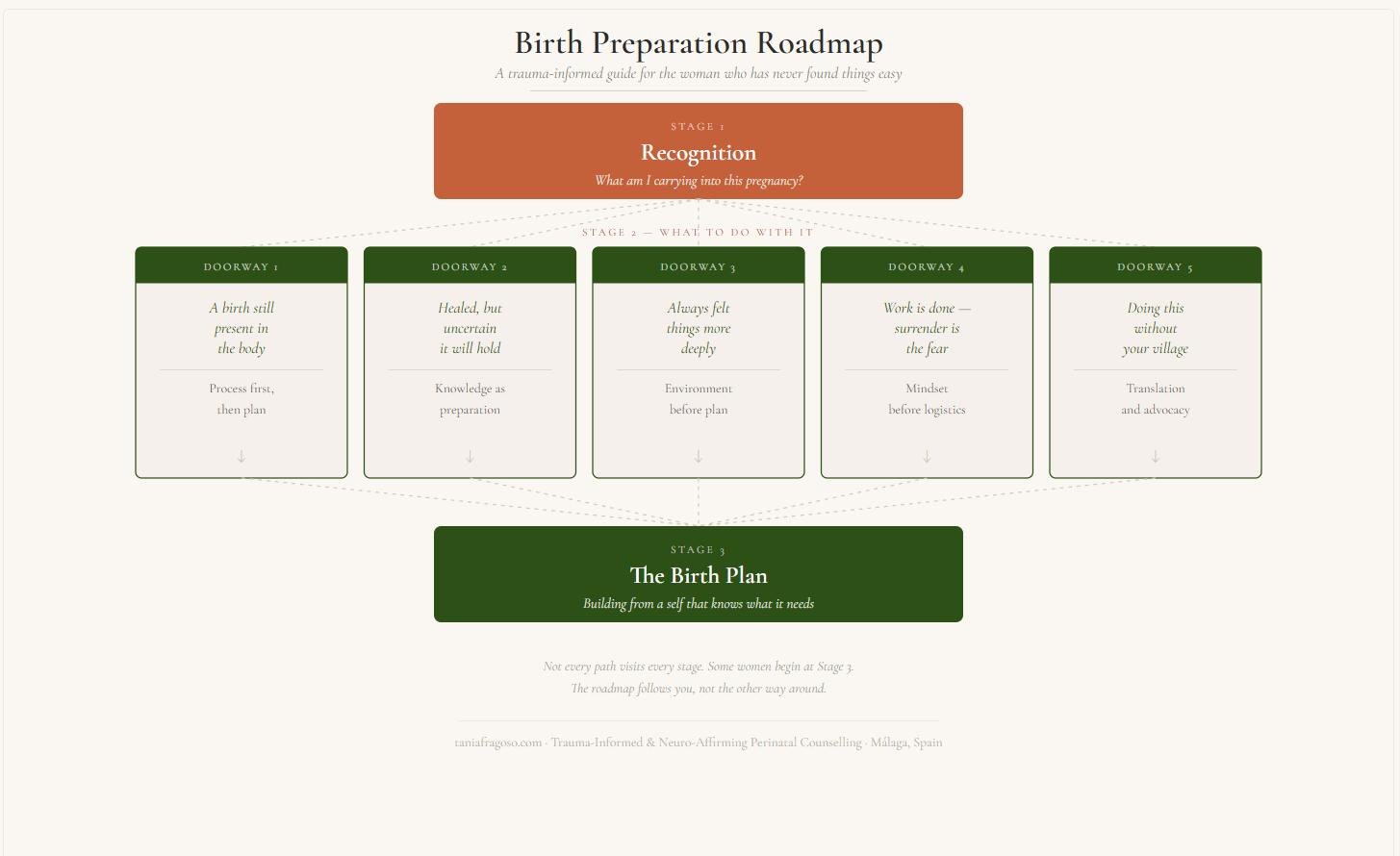
Stage 2 — What Has Surfaced, and What to Do With It
What surfaced in Stage 1 is the starting point, but it does not mean the journey is written in a straight line that you have to follow. If you have read this far, you already know there is no standard advice for a journey that is uniquely yours.
If what surfaced is a previous birth experience still living in the body
The work begins there, not with a new plan. We look at the story at a pace that feels safe to you. Processing what happened, integrating it at a nervous system level, so it cannot be re-triggered at the moment you most need to be present. Only then does the planning begin.
When the woman who had experienced birth trauma arrived, the one with a story she whispered with uncertainty, she would often say something like: “ My birth was not what I expected, but I probably should not call it traumatic, because I know people who had it worse.“ I listened. I reflected back what I heard. And in the silence that followed, she could hear what I heard too.
The validation she was reaching for was not what she needed. What she needed was acknowledgement, and when it came, it was always followed by something she barely noticed at first. A slow release. The breath she had been holding since the delivery room.
Once we knew what she was carrying, we could begin the work. To process the story. To integrate it in a way that would not be re-triggered at the moment of a new birth. This approach is rarely quick, and it’s rarely linear. But there is a framework I return to, which was built on my knowledge of trauma, and on tools like 3 Steps Rewind, that works in three parts: understanding what her trauma response looks like and how it can be re-triggered; processing the original experience at a level the nervous system can absorb; and equipping the people around her, be it her birth partner, or her support team, to recognise the signs and bring her back to the present moment when she needs it most.
If what surfaced is something older than the birth. Trauma that predates pregnancy, healed but uncertain
The work is about understanding what a trauma response looks like in your own body. You may not have experienced birth before, but your body has probably given you a glimpse into how you handle stressful situations. Once you learn to read the signs, you can begin to understand what a trauma response might look like in a birth setting, what is likely to call it forward, and what would help you move safely through it, and how your support team can anchor you when you need it. We build this knowledge not as armour, but as preparation.
If what surfaced is the recognition that your nervous system has always been wired this way
Too sensitive, too feeling, no diagnosis, but no doubt that there is a mismatch between what standard support looks like and what you actually need. Here, the work is environmental before it is practical. Who is in the room, what the room feels like, and what your body will need before it can open. How to ask and advocate for this, and how to communicate these needs in a way that they will be acknowledged and upheld before the day, so you can let go of every version of yourself except the one that is truly you. And if you are not yet confident of what this looks like, we can travel that road too, gently, slowly, and safely.
If what surfaced is the confidence that the past is processed, but the surrender is the fear
There is the woman who has done the work. She healed her past, not superficially, but properly. She sat with it, she processed it, and she made herself a quiet promise: that she would always protect herself, and that she would do whatever she needed to keep those dark days at bay.
She does not arrive uncertain. She arrives informed, and she wants more information. She wants to know her options. She wants to understand what her triggers look like from the outside, so she is not leaving her nervous system to chance at the moment it matters most. She is willing to do the mindset work alongside the practical planning.
And then birth asks her to surrender.
This is the part no one adequately prepares her for. Her past taught her that control kept her safe. That anticipation protected her. That knowing what was coming gave her the half-second she needed to hold herself together. She built something solid from that knowledge, and it has served her. But birth moves through the body on its own terms. It does not reward preparation the way other things have. At some point, it asks her to stop steering.
Her negativity bias, the one cemented by years of learning that things go wrong, that the unguarded moment is the dangerous one, will interpret that surrender as a threat. The work here is not undoing her history. It is helping her write a new ending to a familiar story. Not for the birth alone, but for the child who will grow up watching her decide what to do when things are out of her hands.
The work is about revisiting the scripts she is still holding and asking honestly whether they are serving her in the context of giving birth, and to understand what would feel safe enough to allow the surrender that birth calls for.
If what surfaced is the loneliness of doing this without your village
The work is a translation in every sense. Between systems, between expectations, between the woman your mother raised and the woman standing here now. Together, we look at what has been absorbed unconsciously, handed down through generations, and what actually serves this version of you, the one you have been quietly growing, away from the eyes and pressures that shaped the conditioning in the first place.
There is also the woman doing this without a support network that speaks her language, not just linguistically, but culturally. She grew up hearing birth stories from her mother and her aunts. She absorbed, without being taught, what birth looked like in her family, what was said and what was not, what was feared and what was celebrated. She always assumed those stories would be the ones she would one day add to.
And then she moved. For work, for love, for a life she chose, or not. But pregnancy has a way of pulling a woman back toward the roots she thought she had left behind, and she finds herself holding two sets of expectations that do not easily sit together. The teachings she was handed and the reality she is living. What to keep. What to release. What to grieve quietly, because no one around her will understand what it costs to let it go.
Navigating an unfamiliar maternity system is one layer of this. Learning what she is entitled to ask for, in a language that may not be her first, with a care team who may not know her cultural frame of reference, the work here is practical, and it can be done. But underneath it is something more personal: the task of building her own version of the story her mother told, in a place her mother has never been, without the village that was supposed to be there.
This support is about building a map that connects all these realities, the inherited and the chosen, the familiar and the foreign, in a way that feels right for the life she is actually living now.
If you have found yourself in any part of this, the Birth Preparation Roadmap is where the thread continues. It will take you through each stage, including the one that is yours, and into the practical preparation tools I have used with clients for seven years, including the birth plan and birth support plan templates I built from my own experience and theirs.
Stage 3 — Building the Birth You Are Preparing For
By the time you reach this stage, something has shifted. Not everything, as birth does not ask for certainty, and anyone who promises you that is selling something. But you have looked honestly at what you are carrying, and you have begun to do something with it. That is not a small thing.
Stage 3 is where the practical preparation begins. The birth plan. The birth support plan. The conversations with your midwife. The sensory considerations. The briefing for your birth partner or birth companion. The questions you want answered before you are in a labour room, trying to find your voice.
For most women, this stage feels like relief. After the interior work of Stages 1 and 2, there is something that feels grounding about making a list, naming a preference, and writing down what you need. This can only stem from a self that knows what it needs.
What this stage looks like depends on what surfaced before it.
If you have processed a previous birth experience, the plan you build now is not a correction of the last one. It is something new, something that is written from a different place in your nervous system, without the weight of an unprocessed story underneath it. The traumatic birth you survived does not write this one. You do.
If you are carrying older trauma into pregnancy for the first time, the plan includes more than logistics. It includes what your distress looks like from the outside, and what you need the people around you to do when they see it. It includes the grounding tools you have practised, named and ready, not improvised in the moment. It includes a conversation with your maternity team about your history, as much or as little as feels right, so that the room is prepared before you arrive in it.
If your nervous system is wired for intensity, the plan begins with the environment. Light, sound, who speaks and when, what touch is helpful and what is not, and whether you want the room quiet or filled with something familiar. These considerations are essential for a nervous system that receives input differently, and giving birth requires a nervous system that is not overwhelmed. Creating the right conditions is how you avoid getting there.
If surrender is what you are working with, the plan includes permission, written by you in advance, for yourself. Permission to let go of the version that controls everything. Permission to receive support. Permission to not know what comes next and stay in the room anyway.
If you are navigating a foreign maternity system, the plan is also a translation document. What you need, in the language that the healthcare team can follow. What your rights are, named clearly. Who advocates for you if you cannot advocate for yourself in the moment.
Across all of these, what’s included in the Birth Preparation Roadmap is where this stage becomes concrete. They were built from seven years of sitting with women before their births, mine included, and they account for trauma history, sensory needs, consent preferences, birth partner briefing, and the moments that standard birth plans do not reach.
This is not the end of the preparation. Birth will do what it does, and no plan survives contact with a body in labour entirely intact. But a woman who has done Stages 1 and 2 and arrived at Stage 3 is not the same woman who would have walked into that birthing room without any of this. She knows what she is carrying. She has done something with it. And she has written down, in her own words, what she needs from the people around her.
And then, you let go.
Birth doesn’t follow a plan, but in creating one, you get to know yourself better and allow for a different kind of surrender.
Frequently Asked Questions
What is trauma-informed birth preparation, and how is it different from standard antenatal classes?
Standard antenatal classes prepare you for the physiological process of childbirth. They cover what to expect during labour, pain relief options, and caring for a newborn. Trauma-informed birth preparation starts earlier and goes deeper. It begins with what you are already carrying — a previous traumatic birth, older trauma, anxiety, a nervous system that has learned the world is unpredictable — and works with that material before it gets to the birth plan. The preparation accounts for how your body responds under stress, what your distress signals look like, and what the people around you can do to support you rather than inadvertently re-trigger you. For many women, particularly those who are neurodivergent or have a trauma history, standard classes answer questions they are not yet asking. Trauma-informed care in birth preparation meets them where they actually are.
Can a previous traumatic birth affect how my body responds in a future pregnancy and birth?
Yes, and this is more common than most maternity settings acknowledge. A traumatic birth — one that left you frightened, unheard, out of control, or in physical distress — can create a post-traumatic stress response that sits quietly until the next pregnancy reactivates it. You may find yourself avoiding thinking about the birth, feeling unexpectedly distressed during routine appointments, or noticing that your anxiety about giving birth again feels disproportionate to what you can rationally explain. This is not weakness or overthinking. It is the nervous system doing exactly what it learned to do to protect you. Processing the original experience before preparing for a new birth — rather than trying to plan around it — is the approach that allows the body to actually come with you into the next birth rather than staying, partly, in the last one.
What does PTSD in pregnancy look like, and how do I know if it applies to me?
Post-traumatic stress disorder in the perinatal period is underdiagnosed, partly because it does not always look the way people expect. It does not require a dramatic event. It can follow a birth that was medically routine but felt frightening, out of control, or violating. Common signs include intrusive memories or flashbacks of a previous birth or other traumatic experience, avoidance of anything that brings the memory closer — including pregnancy appointments — emotional numbness or detachment, hypervigilance, and difficulty sleeping. In pregnancy, these symptoms can be intensified by the physical reminders of the approaching birth. If any of this feels familiar, it is worth naming it — to yourself first, and then to someone who can help you work with it rather than through it. A diagnosis is not required to receive support. The experience is enough.
How do I prepare for birth when I have a history of trauma that has nothing to do with a previous birth?
This is one of the most important questions women ask, and one of the least addressed in standard birth preparation. Trauma that predates pregnancy — childhood experiences, medical trauma, sexual trauma, cumulative relational trauma — can show up in the birth room in ways that feel disconnected from the birth itself. The physical exposure of childbirth, the loss of control, the presence of strangers in a clinical environment, the intensity of sensation — all of these can activate a trauma response that has nothing to do with the baby being born and everything to do with what the body has learned about safety. Preparation in this context is about understanding your own trauma response well enough to recognise it when it arrives, building grounding tools you have practised in advance, and briefing your birth partner and midwife clearly enough that they can support rather than inadvertently intensify the distress.
What should a birth plan include for someone with anxiety, a trauma history, or a neurodivergent nervous system?
More than a standard birth plan, and in a different order. Where most birth plans begin with practical preferences — pain relief, positions, cord clamping — a trauma-informed or neurodivergent birth plan begins with what safety requires. That means: who is allowed to touch you and how; what you need to be told before any examination or intervention; how your distress signals present and what you need when they appear; what the environment needs to feel like for your nervous system to remain regulated; what your birth partner's role is and how they can advocate if you cannot find your voice. The practical preferences come after this foundation is laid, not before. A birth plan that begins with the environment and the consent framework — and saves the clinical decisions for once those are established — is a plan that has been built for your actual nervous system rather than a hypothetical one.
How does being neurodivergent affect birth preparation, and what does neuro-affirming support actually look like?
Neurodivergent women — those with ADHD, autism, or both — often find that the standard approach to pregnancy and birth preparation is written for a neurotype that is not theirs. The information is too generic, the environments too sensory, the communication style too indirect. A neuro-affirming approach takes your specific sensory profile seriously — not as a complication to be managed, but as a genuine source of information about what your body needs in order to feel safe enough to give birth. It means building a sensory plan alongside a birth plan. It means practising communication scripts in advance rather than expecting yourself to advocate clearly in the middle of labour. It means naming executive function needs explicitly — including what happens to your decision-making capacity under stress — and building a support structure around those needs rather than hoping they will not show up. Neuro-affirming birth preparation is not adapted standard preparation. It starts from a different place entirely.
How can my birth partner support me if I have a trauma history or a sensitive nervous system?
A birth partner supporting someone with a trauma history or a neurodivergent nervous system needs more than the standard instruction to be present. They need to understand what your distress looks like from the outside — because when you are in it, you may not be able to tell them. They need to know what to do when they see the signs: whether that is grounding you with a specific phrase or touch you have agreed on in advance, advocating with the medical team, or simply creating stillness in the room. The birth support plan I have developed specifically addresses this — it is a document written for the people around you as much as for you, giving them language and a role that is concrete rather than reactive. The preparation that happens between you and your birth partner before the birth is often where the most important work gets done.