ADHD Burnout in Mothers: Signs, Causes and Recovery
ADHD burnout in mothers is a state of cognitive, emotional and physical depletion caused by sustained overload — too much sensory input, too many decisions, too much masking, and not enough recovery time. In the postnatal period it typically shows up as sensory overwhelm, executive dysfunction, brain fog, physical symptoms that do not resolve, and cycles of avoidance or hyperfocus. It is not the same as postnatal depression, though the two often coexist, and it does not lift with rest alone. Recovery moves through three phases: crisis, problem-solving, and application.
By Tania Fragoso — AuDHD perinatal counsellor, mother of three, and someone who once kept the house tidy, the twins fed and dressed, and cried in the shower.
I know what it is like to be in the thick of early motherhood and feel as though something is fundamentally wrong with you. Not with the situation, not with the lack of sleep, but with you. I know the particular exhaustion of ADHD burnout — a brain that cannot switch off, cannot find the start of the to-do list, cannot understand why rest does not seem to restore anything.
I did not have a name for it then. I had postnatal depression diagnoses, panic attacks, and a body that never seemed to recover. I treated each symptom as it surfaced and then watched the cycle begin again. It was not until my AuDHD diagnosis, years later, that the picture finally made sense. What I had been living through was not a failure of willpower or character. It was ADHD burnout, and the transition to motherhood had been the trigger my nervous system could not recover from.
If you are here because something in those words landed, this post is for you.
ADHD burnout symptoms: A Quick Self-Check
The most reliable early symptoms of ADHD burnout in mothers are sensory intolerance, executive dysfunction, emotional exhaustion that rest does not touch, and physical symptoms with no clear medical cause.
Read through the list below and notice how many you recognise from the past month:
Ordinary sensory input — the baby crying, the washing machine, being touched — has become unbearable rather than merely irritating
You cannot sequence simple tasks you used to manage without thinking
You feel blank or detached for stretches of the day and cannot recall them afterwards
Headaches, gut problems or muscle tension that investigations have not explained
You are either avoiding everything, or hyperfocusing on one thing while the rest falls away
Rest, when you get it, does not restore anything
If several of these are familiar, it is worth taking seriously rather than filing under ordinary new-parent tiredness. The free self-assessment will tell you which phase of recovery you are currently in and what the first step looks like.
Mothers experience burnout differently from the workplace picture most people have in mind, which is part of why it goes unnamed for so long.
What ADHD Burnout Actually Looks Like in the Postnatal Period
The symptoms that appear in motherhood rarely match what people imagine. It does not often look like lying in bed, unable to move, although it can. More often, it looks like someone who appears to be managing, until suddenly she is not.
Emotional overwhelm and sensory overload
What was once a minor irritation becomes unbearable. The sound of the baby crying while the kettle boils and the washing machine spins. Being touched after a full day of holding, feeding, and carrying. Clutter in the kitchen that feels physically painful to look at.
This is not being dramatic or difficult. Sensory overload is one of the earliest and most reliable signs that a neurodivergent nervous system is approaching collapse. Research confirms that sensory processing difficulties independently predict perceived stress and burnout symptoms, even in otherwise healthy adults. For individuals with ADHD, particularly those who also have autistic traits, sensory sensitivity after birth can be relentless. It is not a weakness to become overwhelmed when your nervous system has had no opportunity to recover.
Executive dysfunction and decision paralysis
Executive dysfunction turns ordinary decisions, like what to eat, where to start, and what the baby needs right now, into tasks that feel genuinely impossible. You walk into a room, and the thought vanishes. You open your phone to check the time, and twenty minutes later, you have no idea what you were doing. You know the baby needs feeding, but you cannot sequence the steps to make it happen.
This is not laziness or a lack of intelligence. It is what happens when the brain's planning and prioritisation systems are depleted beyond their capacity, and it is one of the most misunderstood ADHD challenges of motherhood.
Brain fog, dissociation, and feeling blank
Many ADHD mothers in the months and even years after birth describe a foggy, detached quality to their days. Time passes without registration. Conversations happen that cannot be recalled later. There is a sense of watching yourself from a slight distance, going through the motions without being fully present.
This can be frightening, and it is often misread by partners, by health visitors, sometimes by the caregiver herself, as a sign of not caring, or not having bonded with the baby. It is the opposite. It is what a brain does when it has run out of capacity to process what is happening in real time.
Physical symptoms that do not resolve
Headaches. Gut problems. Muscle tension that no amount of stretching shifts. Dizziness. A fatigue that sits in the bones. Many neurodivergent caregivers pursue medical investigations for these symptoms — and it should always be the first step, because ruling out other causes matters — only to find that nothing diagnosable emerges. When the nervous system is in a sustained state of overload, the body keeps score.
Avoidance or hyperfocus spirals
When the brain cannot cope with the full picture, it narrows. This can look like avoiding tasks entirely — the pile of admin, the unopened post, the text messages that feel impossible to reply to. Or it can look like the opposite: hours spent reorganising the baby’s wardrobe or researching sleep training methods while everything else falls away. Both are signs of a system struggling with ADHD and emotional dysregulation, not signs of poor character.
What Causes ADHD Burnout in Mothers?
ADHD burnout is caused by a sustained mismatch between the demands placed on the brain and the resources available to meet them — and motherhood intensifies every element of that mismatch at once.
For mothers with ADHD, several factors typically converge:
The loss of coping mechanisms
Before having a baby, many mothers with ADHD have built elaborate scaffolding around their nervous system: rigid routines, external accountability, carefully managed sensory environments, carefully rationed social energy. Motherhood immediately dismantles most of that scaffolding. The structures that kept things running disappear precisely when the cognitive demands double.
The invisible labour of maternal decision-making
Every day of motherhood involves an extraordinary number of small decisions — feeding schedules, sleep cues, medical appointments, equipment, safety checks, the weight of being the person responsible for another person’s survival. For a brain that already struggles with decision-making, planning, and task initiation, the daily demands of motherhood are not a minor adjustment. It is a sustained and relentless demand on systems that were already working at capacity.
Sensory overload accumulation
Each sensory demand of motherhood — being touched, the sounds of a crying baby, disrupted sleep, clutter, noise, the feeling of milk or spit-up on skin — is manageable in isolation. The problem is that they arrive all at once, every day, without the sensory recovery time that a neurodivergent nervous system needs to regulate. What accumulates is not dramatic. It is a slow narrowing of tolerance until ordinary sensory input feels unbearable.
Masking without the means to stop
If you have spent decades learning to mask your ADHD symptoms to be read as competent, that performance does not switch off when you have a baby.
In many cases, the pressure to mask intensifies — in front of health visitors, family, other parents, and partners. The performance of competence continues while the reserves that make it possible dissolve.
The hormonal cascade following childbirth
The steepest oestrogen drop of a mother’s life happens in the days and weeks after birth. When oestrogen falls, dopamine function falls with it, and ADHD symptoms worsen. This is not a separate cause — it is the biological accelerant that makes every other factor harder to manage.
A 2024 study published in AIMS Public Health found that executive function deficits directly mediate the relationship between ADHD and burnout, particularly around self-management of time and self-organisation. In other words, mothers navigating ADHD are running each day on depleted executive fuel before motherhood even enters the picture.
A large Canadian longitudinal study of over 2,500 couples found that mothers with probable ADHD had 1.7 times higher odds of postnatal depression and 1.74 times higher odds of postnatal anxiety across the first two years after birth.
It’s rarely the result of one thing. Each of these factors contributes to burnout individually — arriving together, and persisting for longer than the nervous system can hold, they become something the mother cannot recover from without support.
The shift into motherhood, sometimes called matrescence, reshapes identity, routine, relationships, and the nervous system all at once. For most new parents, this transition is demanding. For neurodivergent mothers, it can be destabilising in ways that are difficult to articulate to anyone who has not experienced it.
ADHD brains rely on dopamine-driven systems to regulate attention, motivation, and emotional responses. After birth, dopamine and oestrogen levels shift dramatically. Sleep becomes fragmented. Sensory input multiplies. The executive function demands of caring for a newborn — planning feeds, tracking appointments, switching between tasks at a moment’s notice — land squarely on the cognitive systems that someone with ADHD experiences as most challenging.
Why Neurodivergent Mothers Do Not Collapse — We Corrode
There is a particular pattern I see again and again in the mothers I work with, and it is the pattern that delayed my own recognition of burnout by years.
We do not collapse. We corrode.
The standard image of burnout is someone who cannot get out of bed. For those with ADHD or other neurodivergence, that image is often wrong. Instead, we keep functioning. We keep feeding our babies, answering the work emails, holding the household together, whilst something underneath is slowly dissolving. The floor keeps dropping, but we never actually fall.
Part of this is biology. Many of us have alexithymia, the difficulty recognising and naming our own internal emotional and physical states. If you cannot read the body's early warning signals- the tightness, the dread, the quiet irritation- you cannot respond to them. You override what you cannot perceive. Research now consistently identifies alexithymia as one of the strongest drivers of burnout in neurodivergent adults (Ali et al., 2025), and a large Swedish cohort of people with clinical exhaustion disorder found that alexithymia, ADHD symptoms, autistic traits, prior trauma, and perfectionism were all significantly correlated with symptom severity.
If you have an autistic profile alongside ADHD, you may recognise this as autistic burnout. The two overlap so heavily in mothers that separating them is often less useful than treating the whole picture. The early signs of burnout are the same in both: withdrawal, sensory intolerance, and a loss of capacity that arrives quietly enough to be explained away.
Part of it is masking. If you have spent decades performing a version of yourself that felt acceptable to the world, stopping is not experienced as a choice. A 2024 study found that self-reported camouflaging predicts poor mental health outcomes over and above autistic traits themselves, with women showing a stronger effect than fathers.
And part of it is protectiveness. Your baby very likely carries the same sensitivity, the same wiring, the same squiggly lines you were told were the problem. You promised yourself that it would end with you. So you do not stop. You cannot afford to stop.
I need to state something that I know many of us secretly tell ourselves: that we are failing and we are weak. I know, I said it too. This is factually incorrect, and it is a harmful thought that keeps us from reaching out for support. The collapse you are experiencing is a well-documented neurological and psychological pattern, and it is why ADHD burnout in mothers so often goes unrecognised — by clinicians, by partners, and most devastatingly, by herself. The emotional exhaustion is real, even when nothing on the outside signals that anything is wrong.
What Is the ADHD Burnout Cycle?
The cycle is the repeating pattern in which a neurodivergent person over-extends, depletes, crashes, recovers partially, and then over-extends again — often without recognising that the same cycle is running each time.
For mothers with ADHD, the cycle tends to follow this shape:
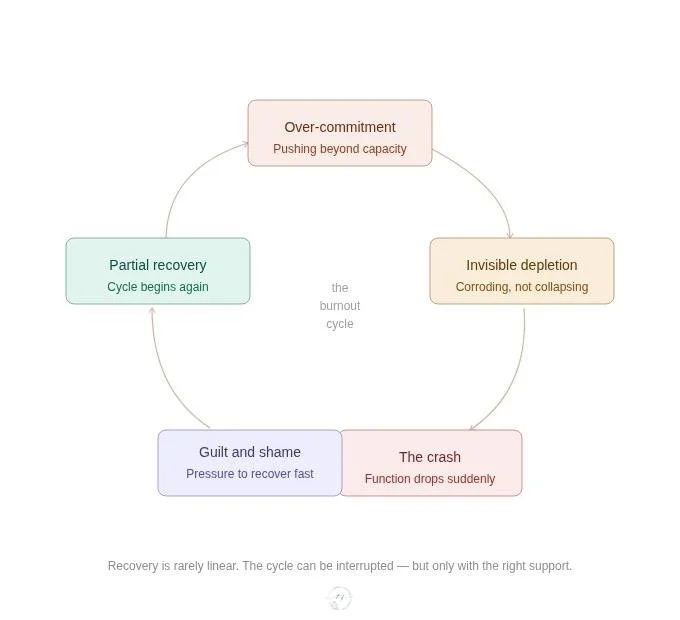
Over-commitment.
The pressure to be capable, to hold the household together, to respond to every need, drives a level of output the nervous system cannot sustain. This is often reinforced by a history of having to work twice as hard as others to appear equally functional.
Invisible depletion.
There is no single moment of collapse. Instead, the capacity to regulate emotions, manage sensory input, make decisions, and maintain the performance of competence slowly erodes. This is the phase most often missed — including by the mother herself, particularly if she has alexithymia and cannot easily read her own internal state.
The crash.
Something stops working. Executive function drops. Emotional regulation fails. The body signals what the mind has been overriding. This is the phase most likely to be noticed by others — and most likely to be misread as postnatal depression, a difficult personality, or a bad week.
Guilt and the pressure to recover quickly.
The crash is often followed by intense shame. The mother who has been performing competently now feels exposed. She pushes herself to recover faster than her nervous system can, driven by guilt about her baby, her partner, or the standard she has set for herself.
Return to over-commitment.
Partially recovered, and believing she should be further along than she is, she re-enters the cycle. Without a framework for understanding what has happened, the same patterns fire again.
What makes this cycle particularly difficult to interrupt in the period after birth is that the structural conditions that drive over-commitment — a newborn, a household, a partner, external expectations — do not pause while the nervous system recovers. Recovery has to happen inside the cycle, not after it. That is why external support and a model of recovery that accounts for the reality of caregivers matter more than willpower. Understanding the cyclical nature is not discouraging — it is the first step toward interrupting it.
How hormones after birth Intensify ADHD Symptoms
This is the part of the picture that is rarely discussed, and it is one of the most important.
ADHD symptoms are closely tied to oestrogen. When oestrogen falls, dopamine function falls with it, and ADHD symptoms worsen. The steepest oestrogen drop of a mother’s life happens in the days and weeks after birth. A 2025 consensus review from the Eunethydis Special Interest Group on Female ADHD confirmed that hormonal transitions, including the period after birth, exacerbate ADHD symptoms and mood disturbances, and that undiagnosed ADHD in caregivers leaves them at particularly increased vulnerability to postnatal depression.
The clinical practice guideline published in the American Journal of Obstetrics and Gynaecology goes further: ADHD symptoms frequently become more challenging to manage during the perinatal period and require additional support. Many also discontinue their ADHD treatment in pregnancy, which compounds the loss.
Your brain is not letting you down. It is navigating a neurochemical storm on less sleep than it has ever had, and the support systems that used to help you cope are often unavailable exactly when you need them most.
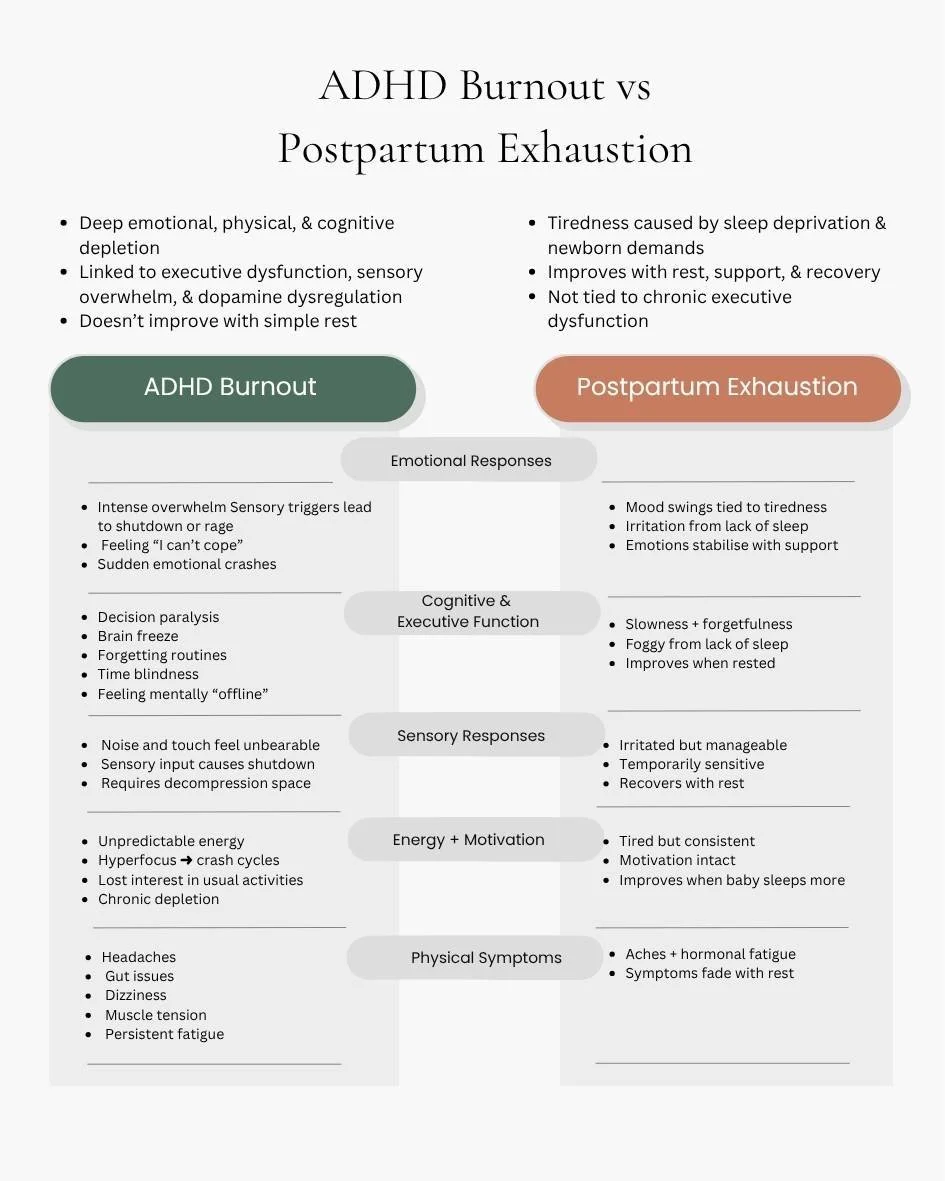
ADHD Burnout or Postnatal Depression? Understanding the Difference
This is one of the most common questions mothers ask, and the honest answer is that the two can look remarkably similar, and they can coexist. Both involve low mood, exhaustion, difficulty coping, and withdrawal from things that used to matter.
The distinction lies in the root. Postnatal depression is primarily a mood disorder linked to hormonal and neurochemical shifts after birth. ADHD burnout is a collapse of the brain's regulatory systems after sustained overload, too much input, too many demands, not enough recovery, for too long.
A mother can have both. And many women who are diagnosed with ADHD only discover it because they sought help for what they assumed was postnatal depression, only to find that the standard treatments- antidepressants, CBT, and talking therapy- helped partially but did not touch the underlying pattern. Attention deficit hyperactivity disorder is still widely imagined as a childhood condition, which is one reason adults with ADHD — women especially — are identified so late, and why many are only recognised after having a baby. If that experience feels familiar, it is worth exploring whether the ADHD layer is part of the picture.
Maternal mental health care that understands both conditions and can hold the complexity of a neurodivergent mother’s experience without reducing it to a single diagnosis is what makes the difference.

How Do You Recover From ADHD Burnout? A Three-Phase Framework
ADHD burnout recovery happens in stages, and the order matters more than the speed.
Most advice about ADHD and motherhood collapses everything into one instruction: rest more. That is not only incomplete, but for many of those with ADHD or other neurodivergence, it is actively unhelpful. “Rest” in the first weeks is a very different thing from “rest” six months in.
The framework I use in my practice is adapted from the Mental Health Standard for Adjustment Disorder, Overstrain and Burnout — a clinical guideline from my counselling training in the Netherlands — reshaped for the realities of neurodivergent motherhood. It has three phases, and trying to skip any of them tends to prolong the time it takes to recover from burnout rather than shorten it.
Phase one: crisis
This is the phase where your body's stress system is no longer producing the hormones it needs to meet daily life. The task is not problem-solving. The task is rest and a significant lifestyle adjustment.
In practice, for a caregiver, this looks like:
Reducing sensory input wherever possible — quieter home, softer lighting, permission to wear earplugs
Permitting yourself to unmask at home
Cancelling anything that is not essential
Asking for help with meals, laundry, decisions — not with the baby, but with the infrastructure around the baby.
Sleep whenever possible, without guilt.
The mindset of this phase is survival, not optimisation. You are not meant to be productive here. You are meant to be held.
Phase two: problem-solving
Once you have stabilised, this is the phase where we begin to understand the patterns that led here. For neurodivergent caregivers, that is not a generic exploration of "stress triggers." It is a specific examination of:
Which parts of your life require you to mask, and what has been the cost of that masking.
How your monotropic attention — the ADHD tendency to deep-focus on one thing — has shaped your over-commitment patterns
How your sensitivity to rejection has driven people-pleasing
How your hormonal cycle interacts with your capacity
What you learned in childhood about your own needs
This is insight work, and it is rarely comfortable. But without it, recovery becomes a loop, recovering, crashing, recovering again, with the same patterns firing each time. According to a 2025 systematic review, the factors most strongly supporting recovery in neurodivergent adults include a more accurate framework for self-understanding, meeting needs for rest and sensory relief, and having individual and community support.
Phase three: application
This is the phase where you begin, slowly and imperfectly, to apply what you have learned. It is not a return to "normal." For many neurodivergent caregivers, "normal" was the environment that caused the burnout in the first place.
This phase is about redesigning your life and implementing systems that work with your nervous system, not retraining your nervous system to fit your life. It might involve renegotiating work arrangements, changing how you handle social obligations, learning new tools that support emotional regulation, setting up sensory-protective routines that become permanent rather than emergency measures, and identifying the people and communities where you can be yourself without performance.
Recovery here is not a before-and-after. It is a slow, deliberate rebuilding.
How Can You Prevent ADHD Burnout?
The most effective way to prevent burnout is to treat early depletion as the signal rather than waiting for the crash. You cannot always avoid burnout entirely, particularly when the demands are structural rather than chosen, but the gap between early depletion and collapse is where intervention works best, and it is wider than most mothers think.
For individuals with ADHD, this means learning to spot the early signals: taking on too much without adequate recovery time, time management becoming increasingly difficult, physical and emotional exhaustion that rest does not resolve, and a growing sense that something is dissolving underneath the surface of daily functioning. ADHD burnout often develops gradually rather than suddenly — and that gradual quality is precisely why it is missed.
Practical risk reduction looks like:
Building deliberate recovery time into each week, not just each day
Reducing sensory load proactively, before it accumulates to the point of overwhelm
Treating masking as a limited resource that needs to be rationed, not a permanent performance
Having a practitioner or trusted person who knows your baseline and can reflect when things are shifting
Burnout cannot always be avoided. But the gap between early depletion and complete collapse is where intervention is most effective — and widest.
Managing Executive Dysfunction in Motherhood
Recovery does not happen in a vacuum. Whilst you are moving through the phases, you still have a baby, a household, and the ordinary demands of life. Executive function support for ADHD mums needs to be external, visible, and forgiving.
A few practices that tend to work:
A whiteboard in the kitchen with today's three priorities. Not ten. Three. Visible to your partner too, so they can help you protect them.
The 90-second start. When a task feels impossible, set a timer for 90 seconds. Commit to that and nothing more. Momentum usually does the rest.
Pre-decided meals. Decision fatigue is real, and it lands hardest on an ADHD brain. Pre-plan, pre-cook, or pre-order whenever you can.
Body-doubling. Having another person physically present, or on a video call, whilst you do a hard task. It is one of the best-evidenced supports for ADHD executive function.
Create simple routines to automate recurring tasks, like restocking nappies, washing baby bottles, pre-dosing water and milk for night feeds and changes.
Borrowing coping strategies from other ADHD caregivers— not because what works for someone else will automatically work for you, but because you do not have to reinvent every tool from scratch.
The goal is to remove as many decisions as possible from the day. This is not self-care in the conventional sense — it is nervous system management. Every decision costs cognitive energy that mothers with ADHD already struggle to spare.
When Standard Therapy Does Not Fit Many Women With ADHD
Many of the parents I support have tried therapy before and found it did not help, or worse, made them feel broken. This is especially common with traditional CBT, which is still the default offering in most perinatal mental health services.
CBT has real strengths, but it makes several assumptions that often do not hold for neurodivergent clients:
That you can accurately read your own internal states (difficult with alexithymia)
Those thoughts drive feelings (often true, but in sensory-dominated nervous systems, the body leads)
That "maladaptive" thinking is the problem (when frequently, the environment is the genuine problem)
If CBT has not worked for you, it does not mean you are beyond help or too self-aware. It means the model was not built for you. What to look for instead:
Trauma-informed care — practitioners who understand that masking and burnout are trauma responses, not character traits.
Neuro-affirming care — practitioners who do not pathologise ADHD or autistic traits but help you work with your nervous system.
Somatic approaches — approaches that work with the body, particularly useful when alexithymia makes purely cognitive work difficult.
You deserve support that meets you as you are.
What Happens If ADHD Burnout Is Not Addressed?
This is the question I was never able to find an answer to when I was in the middle of my own burnout, and it is one I think caregivers deserve an honest response to.
Research on the long-term consequences of untreated burnout is still developing, but the evidence consistently points in one direction.
It becomes chronic. A systematic review of nearly 4,000 neurodivergent adults found that burnout typically becomes a recurring condition with intermittent crises rather than a single episode, with each recurrence often worse than the last.
Skills can be lost long-term. The loss-of-skill feature of neurodivergent burnout, capacities you used to have, become inaccessible and can become persistent when recovery is repeatedly interrupted.
It can progress to clinical exhaustion disorder. In Sweden, where advanced burnout is recognised as a medical diagnosis, clinical exhaustion disorder typically requires years of recovery and is associated with sustained cognitive impairment, sleep disturbance, and high rates of comorbid depression and anxiety.
Physical health consequences follow. Sustained stress dysregulation is linked to increased cardiometabolic risk, including obesity, diabetes, and hypertension in people with ADHD.
Suicidality risk rises. The foundational research on neurodivergent burnout identifies increased suicidal ideation and behaviour as a significant risk, which is why this cannot be left unaddressed.
I share this not to frighten you. I share it because you have likely been told that burnout is something you "just need to push through," and that framing has real consequences. It is a medical and psychological reality that deserves proper care.
If you are recognising severe burnout in yourself rather than early depletion, this is the point to find a professional who can help, rather than waiting to see whether it lifts on its own.
How Perinatal Mental Health Care Can Better Support Mothers With ADHD
Most standard postnatal care was designed for neurotypical nervous systems. The assumption is that with rest, emotional support, and perhaps some medication, a mother will find her feet. For neurodivergent caregivers, that model often misses entirely.
What care that fits ADHD caregivers looks like:
Recognising ADHD as a risk factor for postnatal depression (PPD), not a separate issue to be managed elsewhere
Screening for ADHD in women and mothers presenting with PPD, anxiety, or burnout that has not responded to standard treatment
Sensory-aware environments in clinical spaces, quieter waiting rooms, dimmable lighting, and written information alongside verbal
Executive-function-aware communication, like written summaries after appointments, reminders that do not rely on memory alone
Collaborative planning that treats the parent as the expert on her own nervous system
Practitioners who are trained in both perinatal mental health services and neurodivergence, not one or the other
This is the model I offer in my practice, and it is the model more perinatal services are beginning to adopt. If you have felt unseen in standard perinatal care, you are not imagining it. The gap is real, and it is slowly beginning to close.
Frequently Asked Questions
These are the questions carers with ADHD ask me most often — how long burnout lasts, how it differs from ordinary postnatal exhaustion, whether it means they are failing, and what recovery actually involves.
How long does ADHD burnout last in mothers?
There is no single answer, and that can be hard to hear when you are in the middle of it. Recovery depends on how long the overload has been building, what support is available, and whether the underlying neurodivergent needs are being addressed — not just the symptoms. With the right, brain-compatible support, many begin to notice a shift within weeks. Without it, burnout can persist for months or quietly become the new baseline.
Does ADHD burnout mean I am failing as a mother?
No. It is not a character flaw or a measure of how much you love your child. It is what happens when a nervous system that was already working harder than most — masking, regulating, compensating — runs out of resources. The fact that you are here, trying to understand what is happening, is evidence of the opposite of failing.
What is the difference between ADHD mum burnout and regular exhaustion?
Regular new-parent exhaustion improves with rest. Burnout does not, because the issue is not a lack of sleep alone — it is a collapse in the brain’s capacity to regulate attention, emotion, and sensory input. Rest helps, but it is not sufficient on its own. Recovery requires reducing the demands on the systems that are depleted: sensory load, decision-making, masking, and emotional labour.
Do ADHD symptoms often intensify in motherhood?
Yes, and this is more common than many people realise. Motherhood and ADHD intersect in a way that often reveals traits that were previously masked by structure, routine, or sheer effort. Many women are first identified or diagnosed in the perinatal period precisely because the demands of new parenthood expose what was hidden before. If you are recognising yourself in these descriptions for the first time, that recognition itself is meaningful — and it changes how you can live with ADHD, rather than simply surviving it.
Are there considerations for ADHD medication whilst breastfeeding?
This is an important and nuanced conversation that needs to happen with your prescribing clinician, ideally one with specific experience in perinatal psychiatry. Current clinical guidance suggests that decisions should balance the risks of medication with the risks of managing ADHD unmedicated during pregnancy and postpartum, which are themselves significant. I do not prescribe or advise on medication, but I can support you in preparing for that conversation with your clinician.
What does recovery from ADHD burnout actually look like?
It rarely looks like a dramatic transformation. It looks like the days when you want to throw in the towel, and you do not. It looks like new skills learned slowly, boundaries placed carefully, and needs finally taken seriously. It looks like building a life that fits you, rather than breaking yourself to fit a life that was never designed for you.
You Are Not Alone in This
ADHD burnout in mothers is far more common than most people realise, and it is not a reflection of how much you love your child or how hard you are trying. It is the predictable outcome of a nervous system that was never resourced for the environment it is trying to survive.
If you would like to identify which phase of recovery you are currently in, the free self-assessment is the gentlest place to start — no email required to see your result.
You do not have to figure this out alone. The framework exists. The support exists. And the version of motherhood that fits your nervous system is possible — not perfect, but yours.