RSD and Birth Trauma in ADHD and Autistic Mothers

RSD and birth trauma, and why so many neurodivergent mothers suffer in silenceThere is a particular kind of woman who arrives at motherhood already carrying more than anyone can see.
She has spent years learning to read the room before she enters it. To scan faces for signs of disappointment. To shrink herself just enough to avoid the feedback she fears most, and keep her RSD at bay. She has been called sensitive, dramatic, and difficult, and she has learned to perform otherwise, at enormous cost to herself.
Then motherhood arrives. And the performance collapses.
For many women with ADHD or autism, the postpartum period is the moment everything that was managed, masked, and held together finally gives way. The RSD that was always there, that neurological hair-trigger for perceived criticism, disapproval, or failure, suddenly has nowhere to hide. And if that body has also lived through a difficult birth or early experience, the result can feel not just overwhelming, but completely without explanation.
This post is about that intersection. What happens when RSD and trauma share the same body. How they amplify each other. Why they are so often mistaken for one another. And why so many neurodivergent mothers suffer in silence for far longer than they should.
If you are not yet familiar with it, I would encourage you to start here first: Rejection Sensitive Dysphoria and Motherhood: A Neuro-Affirming Guide. This post builds on that foundation.
How Childhood Trauma Shapes Rejection Sensitivity in ADHD and Autistic Women
It does not appear from nowhere. For many people with ADHD or autism, there is a neurological predisposition; the brain’s emotional regulation system is wired to respond more intensely to social feedback. But neurology alone does not tell the whole story.
Research consistently shows that early experiences of emotional invalidation, being dismissed, criticised, ignored, or simply not believed, teach the body to scan for dismissal before it arrives. A 2024 meta-analysis (Gao, S., Assink, M., Bi, C., & Chan, K. L. (2024). Child maltreatment as a risk factor for rejection sensitivity: A three-level meta-analytic review. Trauma, Violence, & Abuse, 25(1), 680–690. ) found a significant link between childhood maltreatment and heightened sensitivity to rejection, with emotional abuse showing the strongest association of all.
This is not abstract. For many neurodivergent girls, childhood is a prolonged experience of being told that their emotional responses are wrong. Too big. Too frequent. Too much. When that message is repeated across years, across relationships, across every environment where a child is supposed to feel safe, the brain learns. It builds a threat-detection system calibrated for social danger. It begins to perceive actual rejection or criticism as confirmation of what it already fears, even when the cue is ambiguous or neutral.
This can be perceived as a disorder, but in fact It is an adaptation. The body is doing exactly what it was shaped to do.
The difficulty is that the adaptation designed to protect a child in an unsafe environment does not simply switch off in adulthood. It travels. It shows up in relationships, in workplaces, in postpartum wards. And for adults with ADHD or autism who have also lived through chronic invalidation, the fear of dismissal can become so woven into daily life that it feels indistinguishable from personality.
How Masking and ADHD Traits Make RSD Harder to Spot and Treat
One of the most confusing aspects of living with Rejection Sensitivity Dysphoria is that it can look almost identical to trauma from the outside, and from the inside.
Both can involve sudden, intense emotional flooding. Both can include shame, a tendency to withdraw, and a body that fires before the rational brain has caught up. Both can leave a person exhausted, confused about their own reactions, and uncertain whether what they experienced was “bad enough” to take seriously.
For neurodivergent people, decades of masking, performing socially in ways that hide ADHD traits and autistic differences, add another layer entirely. The very strategies that helped a person survive childhood can make it harder for clinicians to see what is actually happening. And when someone has learned to mask distress as well as neurodivergence, even intense emotional pain can go completely undetected.
Understanding the differences, and where they genuinely overlap, matters. Not to put yourself in a box, but because the right support looks different depending on what is actually driving the distress.
It is organised around perceived social threat. The trigger is almost always interpersonal: a comment, a tone, a silence, a look. People who experience Rejection Sensitivity often describe a sudden, intense emotional collapse, dysphoria that arrives before the rational mind can evaluate whether actual rejection has occurred. In people with ADHD or autism, the brain’s emotional regulation system struggles to filter the intensity of social feedback, meaning the alarm fires loudly even when the danger is small or imagined. What might look like an overreaction from the outside is, from the inside, a full-body fear of rejection made real.
Post-traumatic stress disorder (PTSD) is organised around a specific traumatic event or series of events. The body becomes conditioned to respond to reminders of that experience, sounds, smells, physical sensations, and situations that echo the original threat. Symptoms include intrusive memories, nightmares, hypervigilance, and avoidance of trauma reminders.
Complex PTSD (C-PTSD) develops in response to prolonged, repeated difficulty, often in childhood, often within relationships where escape was not possible. In addition to PTSD symptoms, C-PTSD frequently includes intense difficulties with emotional regulation, a persistently negative sense of self, and profound problems with relationships and trust. For many neurodivergent women who experienced chronic invalidation, emotional neglect, or a series of difficult medical experiences, C-PTSD may be a more accurate frame.
Where they converge
For many ADHD and autistic mothers, all three are present simultaneously, and they reinforce each other in a way that makes the combined picture significantly harder to treat than any single diagnosis would suggest. It is worth noting that borderline personality disorder shares several features with this overlap, and misdiagnosis is common, particularly in women whose ADHD traits and difficult early experiences were never properly assessed together.
A difficult birth, for example, can leave the body primed for threat in the postpartum period. When that already-sensitised system then encounters social feedback, a midwife’s tone, a partner’s sigh, a comment about feeding, the RSD alarm does not fire at its usual intensity. It fires through a body already on high alert, already scanning for danger, already depleted. The result is a reaction that feels completely out of proportion, that the mother herself cannot explain, and that can easily be dismissed by others and by herself as instability.
It is neither. It is two physiological responses happening at the same time, in a brain already working harder than most to manage the world. The intense emotional experience that follows is not a character flaw. It is the predictable result of a nervous system carrying more than it was designed to carry alone.
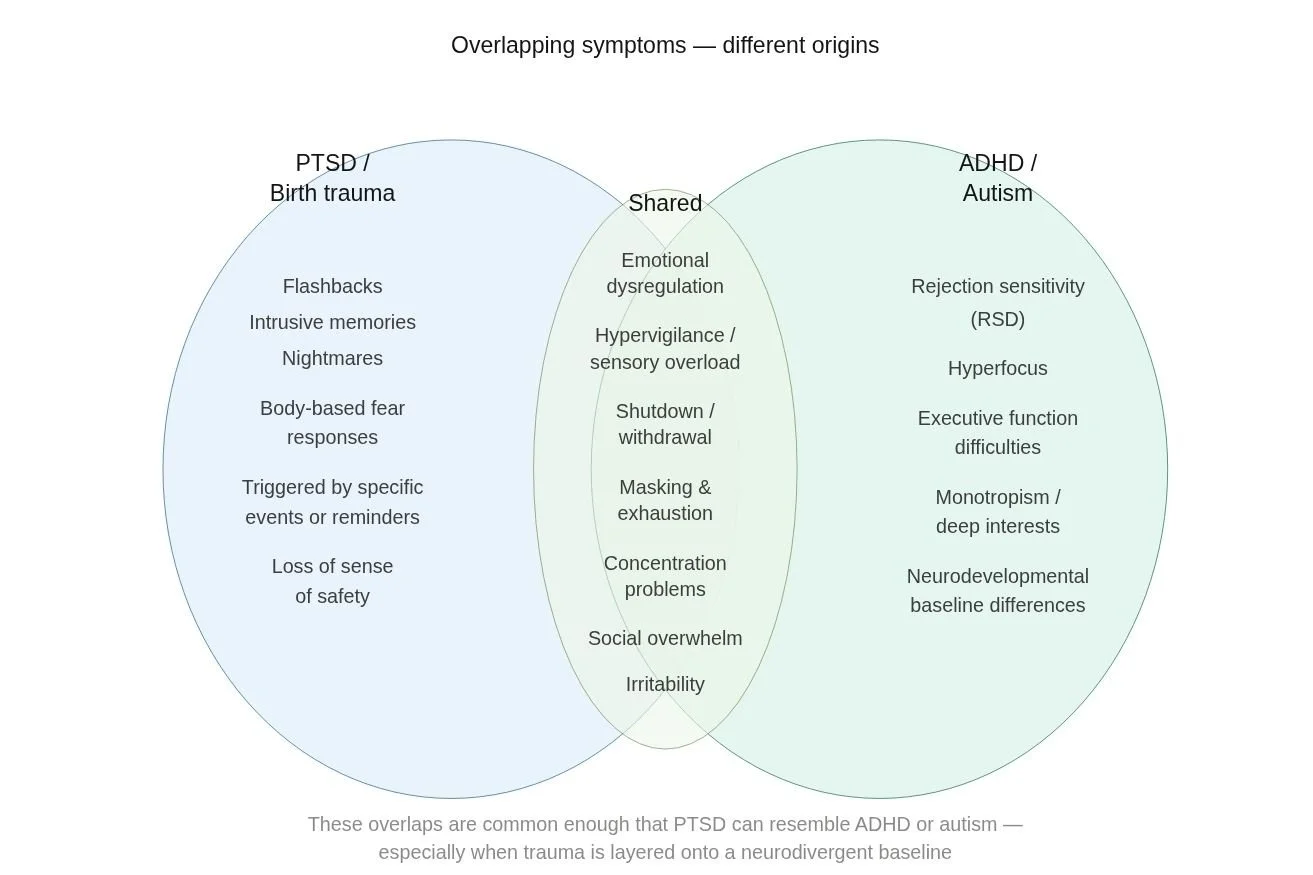
The biggest shared manifestations are emotional dysregulation, sensory overload, shutdown and withdrawal, irritability, concentration problems, and social overwhelm. These overlaps are common enough that PTSD can resemble ADHD or ASD, especially when a difficult experience is layered onto a neurodivergent baseline.
How Birth Trauma Amplifies Rejection Sensitivity in the ADHD and Autistic Brain
Birth trauma does not end at delivery.
For many neurodivergent mothers, what happened in the birth room, the loss of control, the feeling of not being heard, the procedures that happened without adequate explanation or consent, the moments where fear was dismissed or minimised, does not stay in the past. It travels into the postpartum period, embedded in a body that has learned, once again, that it is not safe to trust the people responsible for its care.
Research tells us that autistic women are significantly more likely to report feeling belittled, ignored, and uninformed during childbirth. When a nervous system already primed for sensitivity to rejection enters a high-stakes medical environment, one defined by loss of autonomy, sensory overwhelm, and constant evaluation, the conditions for a traumatic experience are not just possible. They are, for many, almost inevitable.
What happens next is a kind of compounding. The postpartum body is already depleted, hormonally, physically, neurologically. Sleep deprivation alone significantly lowers the threshold for emotional dysregulation. Add a body now, also hypervigilant from a frightening birth, scanning for signs of danger in every interaction, every clinical visit, every well-meaning comment from a family member, and the alarm does not just fire more often. It fires through a system that has no capacity left to absorb it.
This is why so many neurodivergent mothers describe the early postpartum period as a complete unravelling. Not because they are fragile. But because they have been handed the most demanding role of their lives immediately after an overwhelming experience, in a care system that was not designed to notice any of this.
A body that cannot regulate itself cannot offer regulation to another. A nervous system still bracing for impact cannot tell a small, sensitive nervous system that everything is safe. The dysregulation moves through a family quietly, until it is simply how things are.
Why RSD Stops Neurodivergent Mothers from Asking for Help — and What That Costs Their Mental Health
There is a painful irony at the heart of Rejection Sensitivity Dysphoria: the very thing that could help, reaching out, asking to be believed, allowing someone to hold the story, is the thing that makes it feel most impossible.
For neurodivergent mothers carrying both Rejection Sensitivity and a difficult birth history, the barrier to help-seeking is not laziness, denial, or lack of insight. It is a body that has learned, through years of lived experience, that disclosure carries risk.
Consider what asking for help actually requires. It means telling someone you are not coping. It means being vulnerable to their response. And for someone whose brain is wired to perceive ambiguous social cues as threatening, whose alarm fires before the rational mind can evaluate the actual danger, that vulnerability can feel catastrophic.
The internal calculus sounds something like this:
What if they tell me I am overreacting? What if their perception of me confirms what I have secretly always feared, that I am simply too sensitive for this? What if I finally name what happened and they minimise it?
And so the mother stays silent. She keeps the house running, the children fed, and the appointments attended. She performs competence because competence is the armour that keeps the verdict at bay. The emotional drain of this is significant and largely invisible.
For neurodivergent people who have also been told they lack empathy, another misunderstanding rooted in how autistic mothers process and express emotion, the shame runs even deeper. The ability to feel is not the question. The ability to feel, while feeling safe, is.
A 2026 qualitative study (Rowney-Smith, A., Sutton, B., Quadt, L., & Eccles, J. A. (2026). The lived experience of rejection sensitivity in ADHD — a qualitative exploration. PLOS One, 21(1): e0314669. ) found that people who experience Rejection Sensitivity identified childhood interpersonal distress and caregiver dismissal as contributors to their reactivity, and that this same pattern shaped how they navigated help-seeking in adulthood. The fear of being dismissed was not irrational. For many, it was based on direct exposure.
This is particularly significant in the perinatal context, where neurodivergent mothers already report feeling overlooked and uninformed by healthcare providers. When the care system itself has been a source of invalidation, and for many, the birth room was exactly that, asking that same system for support postpartum requires an act of trust that Rejection Sensitivity makes extraordinarily difficult to access.
The silence can be seen as a sign of weakness, but It is just a logical response to a body that has learned, again and again, that it is safer not to speak.
Understanding this changes how we design support. It means that the first task is not to offer information or strategies; it is to create the conditions in which a mother feels safe enough to begin.
“The first task in supporting a neurodivergent mother with RSD is not to offer strategies. It is to create the conditions in which she feels safe enough to speak.”
Trauma-Informed Somatic Support for ADHD and Autistic Mothers: What to Try and What to Avoid
When it is layered with a difficult birth event, standard advice often falls short. Worse, some commonly recommended somatic exercises can inadvertently overwhelm a body that is already on high alert.
Exercises involving prolonged breath holds, closed eyes, full body scans, or progressive muscle relaxation can, for some survivors, intensify dissociation, trigger flashbacks, or push the body outside its window of tolerance. Building tolerance to sensation gradually, titrating rather than flooding, is what makes the difference between settling and retraumatisation.
The following tools are drawn from trauma-sensitive frameworks, including the principles of Trauma Centre Trauma-Sensitive Yoga (TCTSY), the only empirically validated body-based intervention for complex PTSD. They are designed to be brief, choice-based, eyes-open, and externally anchored, beginning with the environment rather than the body.
These are not prescriptions, but a gentle first step. Take what fits. Leave what doesn’t. The goal is not to reframe the emotion or think your way to calm, but to gently shift the body’s physiological state through sensation and orientation.
Orienting to the room
With eyes open, slowly notice five things you can see. Not with effort, just letting your gaze move. This is your body checking that the environment is safe. It is one of the most effective and underused settling tools available.
Feet on the floor
Feel the contact between your feet and the ground. You might press down slightly or notice the texture of the floor. This is external sensation, grounding through contact with something outside the body, rather than directing attention inward.
A slightly longer exhale
Not counted. Not held and not forced. Allow the out-breath to be a little longer than the in-breath. The exhale activates the body’s rest state without requiring focus on breathing itself.
Humming or a gentle “voo” sound
A low, sustained hum on a slow exhale stimulates the vagus nerve directly. One of the fastest routes to returning to baseline is available without professional support.
Gentle movement
Rocking, rolling the shoulders, shaking out the hands. Movement disperses the stress hormones that build during an episode. Any gentle, self-directed movement counts.
Self-touch with choice
If it feels comfortable, place one hand on the upper arm, chest, or cheek. The keyword is if. For those with a difficult history involving the body, this may not feel accessible, and that is completely valid.
Butterfly hug
Crossing the arms over the chest and alternately tapping the upper arms at a slow, comfortable rhythm. Bilateral stimulation with eyes open throughout.
Cold water on the hands or face
Fast, simple, externally anchored. Shifts the body through external sensory input with no internal focus required.
A note on tolerance and timing: These tools work best when used before reaching the peak of an episode, when the body is activated but not yet flooded. Using them socially, in small everyday moments of activation, builds the body’s ability to feel safe more quickly over time. They are not a cure. They are a way of teaching the nervous system, slowly and repeatedly, that it is allowed to settle.
These tools work best when offered with invitational rather than directive framing. You might like to try... rather than close your eyes and breathe deeply. The difference matters enormously for a body that has been overridden before.
You can access a downloadable version of these tools with sensory-sensitive guidance below.

When to Seek Professional Support, and How to Find Someone Who Can Actually Help
The tools above can help in the moment. But they are not a substitute for professional support, and for mothers carrying both Rejection Sensitivity and a difficult birth history, that support needs to be chosen carefully.
Standard talk therapy is often insufficient on its own. The RSD alarm fires too fast and too intensely for cognition to catch up. By the time you are sitting across from someone trying to process what happened, the moment has already passed, and the shame has already settled. Some clinicians explore whether medication may support emotional regulation alongside therapy, a conversation worth having with an ADHD-informed psychiatrist if other strategies alone are not enough. ADDitude Magazine has a useful overview of the pharmacological options currently discussed in clinical practice.
What actually helps is care that works with your neurology rather than around it.
Addressing the birth experience first
For many ADHD and autistic mothers, an unprocessed birth story amplifies the RSD alarm, sensitises the body, and makes everyday feedback land harder than it should. Processing your childbirth story is not a luxury; it is often the foundation for everything else.
A Neuro-Affirming Birth Debrief offers a structured, trauma-informed space to understand the clinical picture and begin to reduce the emotional charge the birth still carries. For those whose birth has left more lasting symptoms, the 3 Steps Rewind technique gently reduces the intensity of those memories without requiring you to relive them in detail.
Perinatal counselling
Sometimes what is needed is not a plan or a technique but a sustained, containing relationship with someone who understands neurodivergent perinatal mental health from the inside.
Perinatal Counselling offers space to process the identity shift of matrescence, untangle the patterns that predate motherhood, and build a more settled relationship with yourself at whatever pace your body allows.
What to look for in any provider
Wherever you seek support, look for someone who is neuro-inclusive, who sees your wiring as a difference, not a deficit, trauma-informed, and experienced specifically with ADHD and ASD in the perinatal period. These are not standard qualifications. Ask directly.
You Were Never Too Sensitive
If you have read this far, something in this will have resonated.
Perhaps you recognise the silence, the years of staying quiet because speaking felt more dangerous than staying stuck. Perhaps you recognise the body, the shallow breath, the braced muscles, the system that forgot how to rest. Perhaps you recognise the alarm, the wave that rises before your rational mind has caught up, the intensity that feels completely out of proportion and completely beyond your control.
None of this is a character flaw. It is not instability, overreaction, or weakness.
It is a body shaped by the years of being told you feel too much, by a birth that overwhelmed your capacity to cope, by a postpartum period that demanded more than any depleted system could give. It is ADHD and ASD in a world that was not designed for either. And it is, underneath all of it, a brain doing exactly what it learned to do, protecting you in the only way it knew how.
The work is not to feel less. It is to reframe what is possible, to find the conditions in which your body finally learns that it is safe to feel, without bracing for the verdict.
That space exists. You deserve to be in it.
And if nobody has said this clearly enough yet: you were not too sensitive. You were under-supported, in a system that did not know what to do with the depth of you.
That is not the same thing at all.
RSD can make it especially hard to sit with what happened during birth without spiralling into shame. In perinatal counselling, we work with both the trauma and the nervous system pattern underneath it, so you're not doing that alone.
Not sure where to start? I offer a free 30-minute introductory call, no pressure, no agenda. Just a gentle conversation to explore where you are in your journey, and whether any of my services feel like a good fit