Perinatal Anxiety in Autistic and ADHD Mothers: When the Worry Won't Settle

Mothers who are autistic and those diagnosed with ADHD have a higher risk of experiencing perinatal anxiety compared to neurotypical mothers, and it rarely presents as straightforward worry. When I was pregnant with my twins, I carried a low hum of dread that was always present, hiding in plain sight below the mask many of us have learned to use so well it becomes imperceptible even to ourselves. Some of us have always lived this way, and it's simply part of who we are. For others, it comes as a surprise. Either way, it comes down to a nervous system built differently meeting one of the most demanding periods of a person's life, leaving you feeling permanently braced for the thing about to go wrong, and creating the assumption that something is fundamentally wrong with you.
It isn't. This is for the mothers who recognise that feeling: autistic, ADHD, both, or simply certain your mind has always worked differently, whose anxiety symptoms during pregnancy or early motherhood never matched the tidy descriptions in the leaflets.
If you'd like the general picture first, what perinatal anxiety is, the usual signs, causes and treatment, I've laid that out in a companion piece. Here, I'm going straight into what's different for us.
Why some of us are more vulnerable
A 2024 systematic review pooling fourteen studies and more than 940,000 participants found a higher prevalence of perinatal anxiety and postpartum depression among women with neurodevelopmental differences across all studies in that review, whether the women had a formal ADHD or autism diagnosis, or were identified through validated questionnaires (Mackintosh, Reed & Jayakody, 2024). So if this is you, the company is considerable, even when it feels lonely.
The same review found the higher rates consistently linked to a handful of factors: unsatisfactory healthcare experiences, low disclosure of diagnosis for fear of stigma, sensory overload in clinical settings, and difficulty with early bonding and breastfeeding. A prior history of mental health conditions such as depression and anxiety, a negative birth experience, and a lack of neurodivergence-informed care increased risk further.
What that tells me is that a good deal of this anxiety is service-shaped rather than person-shaped. Sensory-friendly adjustments, continuity of care, and being believed the first time you disclose a difficulty are not small things. They're some of the most direct levers available for reducing anxiety in women with ADHD and autism.
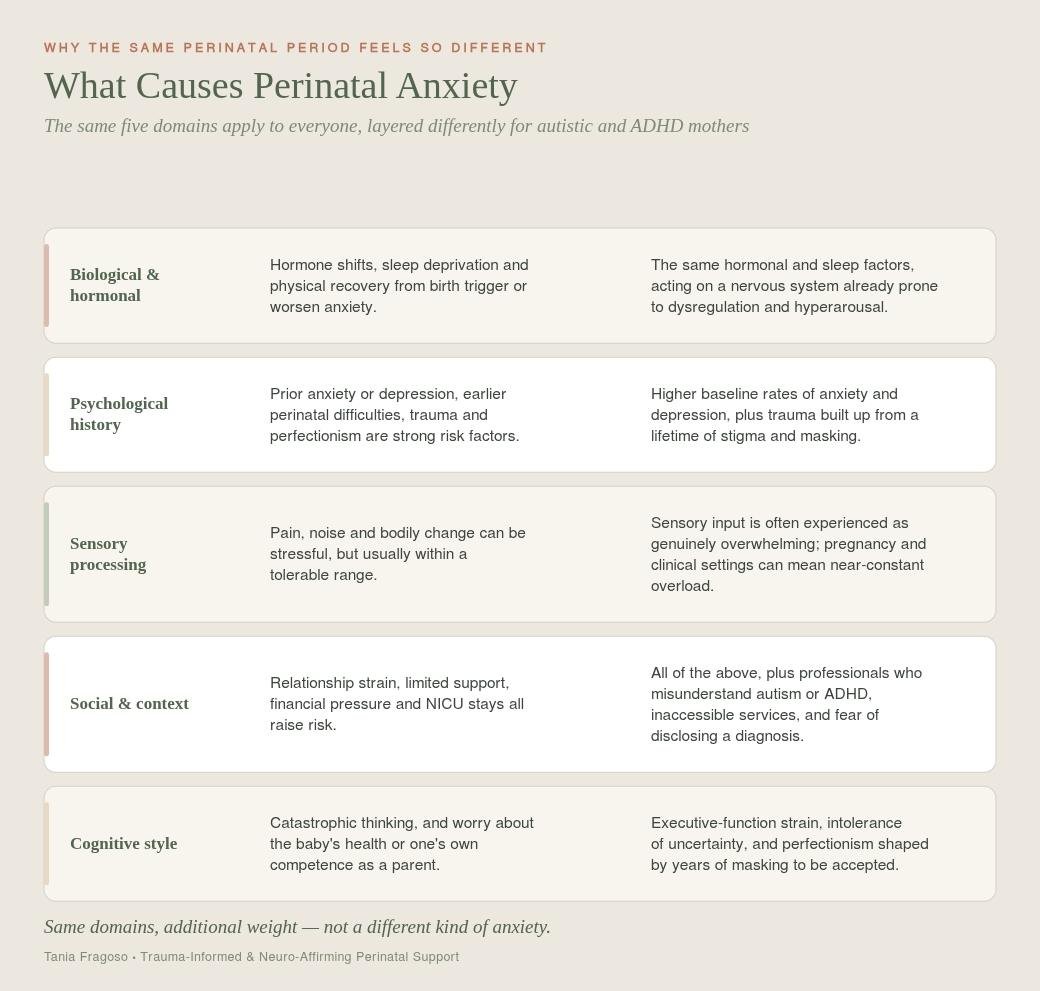
The general causes of perinatal anxiety, hormonal shifts, psychological history, and socioeconomic context are the same ones covered in the companion piece. What changes for autistic and ADHD mothers is how much weight each one carries. The same hormonal shifts land on a nervous system already closer to dysregulation. The same psychological risk factors sit alongside years of masking and stigma. The same social pressures meet healthcare systems that are often unprepared for how we communicate. Sensory processing and cognitive style carry extra weight on top: sensory input that would be manageable for most people can mean near-constant overload, and executive-function strain turns the ordinary unpredictability of new parenting into something much harder to sit inside.
None of this is a different condition. It's the same causes, carrying more weight.
How perinatal anxiety shows up differently in autistic and ADHD mothers
The usual symptoms, racing thoughts, physical tension, and panic, show up here too, but often arrive as restlessness in the body rather than a clear stream of worry. The way anxiety presents is often different, and this is where the general picture stops being much use.
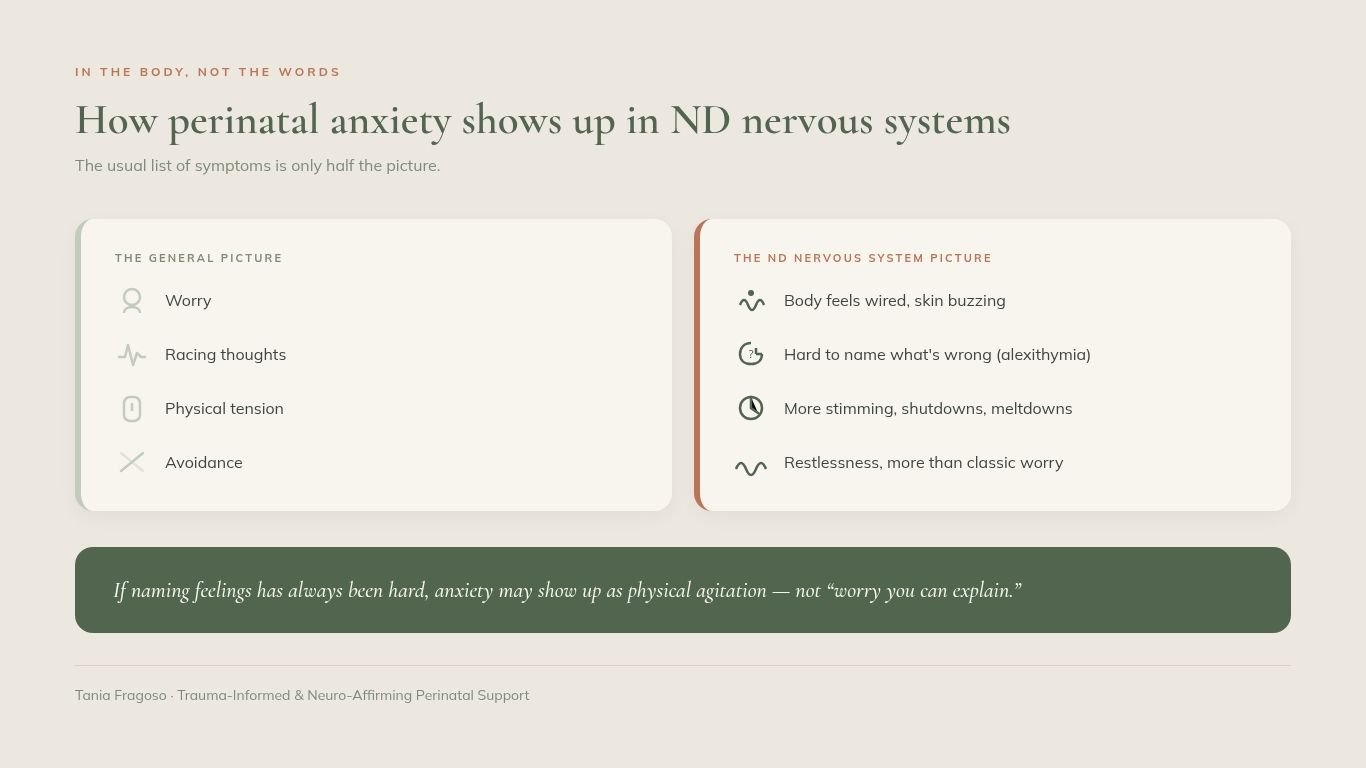
When the anxiety lives in the body, not the words
For many autistic and ADHD new mothers, anxiety arrives first as physical restlessness or agitation rather than a stream of anxious thoughts. You might feel wired, unable to settle, skin buzzing, without being able to say what you're worried about. If naming feelings has always been hard for you, that gap is real and has a name. I've written more about it in Understanding Alexithymia in Autistic and ADHD Mothers, and it's one reason "worry" is often the wrong word for what you're carrying.
The sensory weight of maternity care
Antenatal appointments, scans and delivery rooms are bright, loud, unpredictable places, full of strangers touching you and information arriving faster than you can process it. In a survey of 417 autistic and 524 non-autistic people, autistic participants reported the sensory and physical demands of pregnancy as more overwhelming, found antenatal classes harder to access, and were less satisfied with their relationships with the healthcare services professionals treating them (Hampton et al., Perinatal Experiences I). A follow-up survey looking at childbirth and the postnatal period found the same pattern continuing after the birth (Hampton et al., Perinatal Experiences II). None of that is a minor irritation. For an autistic or ADHD nervous system, it can be the main event, and dread of the environment itself, rather than of the birth or the baby, is common and rarely spoken about, because it sounds, from the outside, like an odd thing to fear.
When the to-do list collides with executive function
ADHD and autistic mothers often hit executive paralysis under this kind of pressure: the antenatal forms, the appointment you keep meaning to book, the hospital bag you cannot make yourself pack. From the inside, it feels like anxiety plus a jammed engine. From the outside, it can be mistaken for not coping or not caring, which it isn't.
If you're already taking medication for ADHD, pregnancy adds another layer to the pharmacological picture. Many women reduce or stop stimulant medication while pregnant or breastfeeding, on medical advice, and the return of untreated ADHD symptoms, on top of everything else, can drive anxiety up considerably. This is under-researched as its own mechanism, but it's a real and common experience worth naming to your prescriber rather than working through alone.
Alongside all of this, you might notice more stimming, more shutdowns or meltdowns, and real distress when a routine changes without warning. It's worth saying clearly: stimming, needing routine, or scripting what you want to say before an appointment are not symptoms to correct. They're how your system regulates itself. The anxiety is the extra load on top, not the neurodivergence underneath.
The beliefs underneath the anxiety
In my counselling work, one of the gentlest and most useful things we do is look for the belief sitting under an anxious feeling, rather than arguing with the feeling itself.
It might sound like "I panic every time she cries because I can't always stop it," and underneath sits a quieter belief: that it's unbearable to be the one who cannot make the distress stop. Or it sounds like "I like to prepare for the worst so I'm ready," and underneath is the belief that the anxiety is the thing keeping everyone safe, so letting go of it feels dangerous.
You don't have to force those beliefs to disappear. Often, just naming them takes some of the charge out. A feeling you understand is easier to sit beside than one that seems to come from nowhere.
Why it wears at your sense of who you are
Anxiety is exhausting on its own. What makes the perinatal version harder is the timing. You're already in the middle of matrescence, the shift into being someone's mother, working out who you are now and grieving parts of the old life you didn't know you'd miss. Anxiety erodes your sense of yourself at the exact moment that self is being rebuilt. That's when the shaming thoughts creep in: everyone else seems to be enjoying this, I must be doing it wrong, my baby deserves better than me. If you want to read more about that identity shift, Postpartum Support for Neurodivergent Parents goes into it properly.
On the fear that being neurodivergent makes you a worse mother, the research is more careful than reassuring, and I'd rather give you the honest version than a tidy one. One study of nearly 2,700 women at one month into the postpartum period found that difficulties with social skills and imagination were linked to poorer scores on a maternal-infant bonding scale, while a stronger attention to detail was linked to better bonding scores, a mixed picture rather than a simple risk factor, and the study describes autistic traits overall as only weakly related to bonding (Fukui et al., BMC Psychiatry). Set against that, research that has watched autistic mothers interact with their babies, rather than relying on self-report scales, has generally found their sensitivity and responsiveness comparable to non-autistic mothers, even when those same mothers report far more distress along the way. Both things seem to be true at once: the anxiety is real, and the picture on bonding is mixed rather than uniformly worse, and neither is a reliable measure of how you are doing with your baby.
A neuro-affirming approach to anxiety in motherhood
The standard treatment picture, CBT, medication where needed, peer support, stepped care, is the same starting point regardless of neurotype, and I've laid that out in full in the companion piece. What's different is what reaches an autistic or ADHD nervous system once you're inside that picture.
There's no single fix, and I'd distrust anyone who offered one. But there are things that do take the edge off, and most of them work by sending your nervous system a signal of safety rather than by talking you out of the fear.
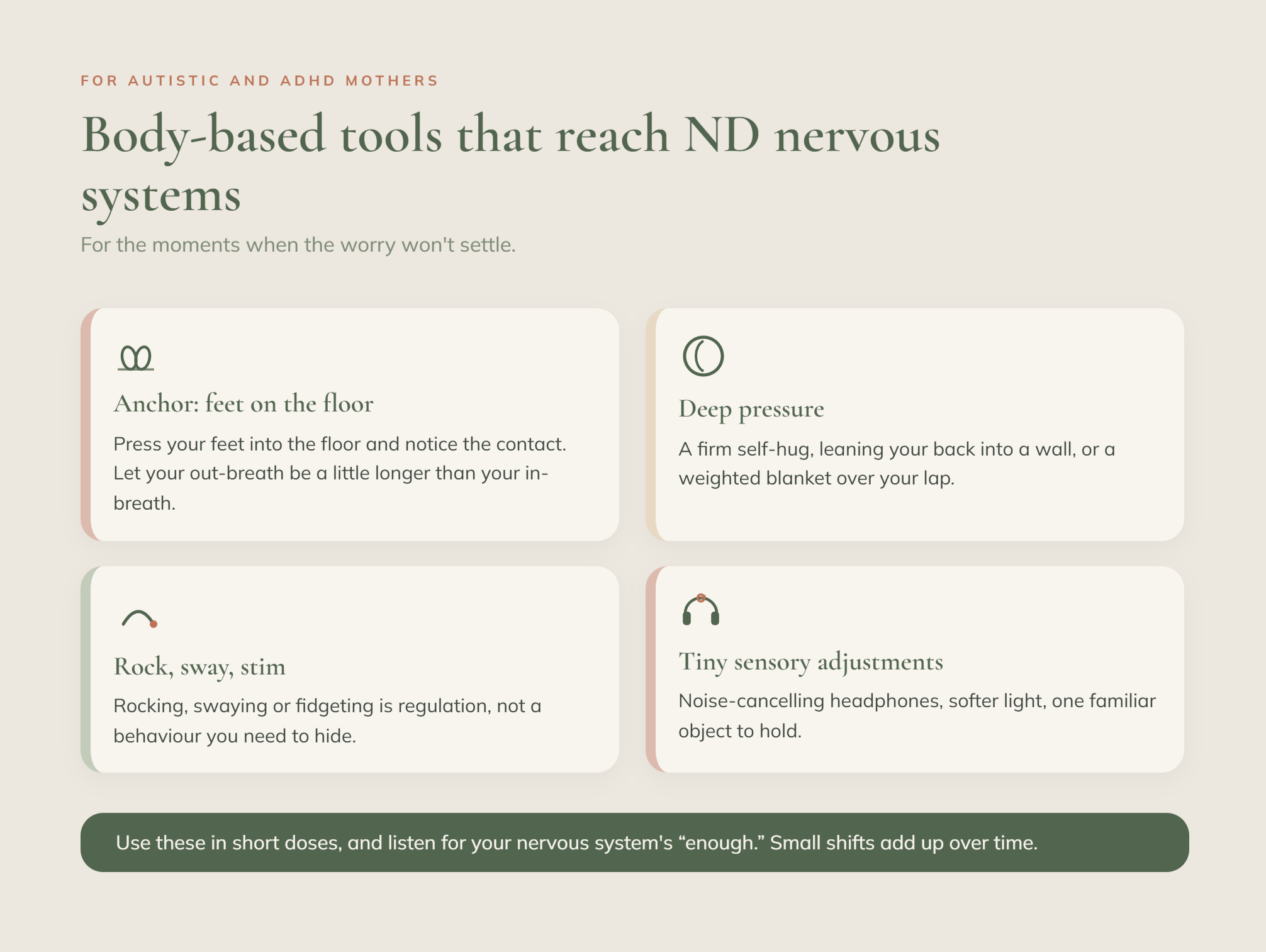
Body-based tools tend to reach us faster than thinking-based ones when we're already overloaded. Pressing your feet into the floor and noticing the contact, then letting your out-breath get a little longer than your in-breath, does something real to a hyper-aroused system. So does deep pressure: a firm self-hug, leaning your back into a wall, a weighted blanket across your lap. If rocking or stimming helps you settle, use it without apology. It's regulation, not something to hide.
Where you have any say in your care, small adjustments matter more than they should have to. You're allowed to ask for dimmer lights, information in writing, the same midwife where possible, a moment before you answer. Scripting these requests in advance, or bringing someone who can advocate for you, is sensible, not a failure to manage
And there's the quieter work: understanding the belief under the feeling, and talking it through with someone who listens and reflects, rather than rushing to fix you or, just as unhelpfully, leaving you stuck in the story. For some mothers that's a trusted friend. For others it's a counsellor who understands both trauma and neurodivergence.
Below is a small tool I made for exactly these moments. It has a gentle mood check-in with room for "not sure," a breathing pacer you can slow right down, and a few body-based prompts for when your thoughts are racing. Nothing is timed, nothing is scored, and you can close it whenever you like. Come back to it before an appointment, in the small hours, or any time the worry won't settle.
When to reach for more support
Some anxiety in pregnancy and early parenthood is expected. It's worth speaking to your GP, midwife or health visitor when the worry stops easing, becomes more constant rather than less, or starts shaping your daily life. Intrusive thoughts that frighten you, or any thoughts of harming yourself or your baby, are a signal to reach out straight away rather than wait. These are more common than people admit, and they're treatable. If your anxiety is moderate or severe, your GP can refer you to a specialist perinatal mental health service, and it's important to seek help early rather than to see if it settles on its own.
A quick reassurance, because it stops many mothers from asking: telling a professional you're struggling does not mean your baby will be taken from you. It means you get information and support. Alongside my own work, PANDAS Foundation runs a helpline for exactly this kind of perinatal distress, if you'd like a first conversation that isn't with me.
Frequently asked questions
A few of the questions I'm asked most often about perinatal anxiety in autistic and ADHD mothers are answered directly.
What are the risk factors for perinatal anxiety in neurodivergent mothers?
The clearest ones, drawn from the research above, are a prior history of mental health issues like anxiety or depression, previous birth trauma, sensory overload in clinical settings, unsatisfactory healthcare experiences, low disclosure of a neurodivergent diagnosis, and a lack of neurodivergence-informed care. Several of these are about the systems around you rather than anything about you, which is worth raising awareness of.
Why does anxiety feel so much worse around midwife or hospital appointments?
For many autistic individuals and those with an attention deficit hyperactivity disorder diagnosis, the appointment setting is as much the trigger as the appointment itself. Bright lights, noise, unpredictability, strangers, physical examination and fast-moving information are a heavy sensory and processing load. Dreading the environment is a reasonable response to it, and you're allowed to ask for adjustments that make it more bearable.
Should I tell my midwife or GP that I'm autistic or have ADHD?
That's your call to make, and there's no single right answer. Disclosure can open the door to real adjustments, dimmer lighting, written information, and more processing time, but many mothers stay quiet out of a reasonable fear of being judged less capable. If you do disclose, it's worth being specific about what would help, rather than leaving a professional to guess.
How do hormonal changes affect ADHD symptoms during the perinatal period?
Often for the better, at first. Rising oestrogen through pregnancy supports dopamine function, and some women find their ADHD symptoms during pregnancy ease over these months. The shift after birth tends to go the other way: oestrogen drops sharply within days of delivery, and ADHD symptoms commonly return, sometimes more intensely than before pregnancy, right as the lack of sleep and a newborn's demands are at their peak. It's worth knowing this in advance rather than being blindsided by it.
What support services are available for perinatal anxiety in ADHD or autistic mothers?
Standard perinatal mental health teams can support the anxiety and depression side of things, but ADHD itself often isn't something they treat directly. Some NHS trusts state outright that while they'll work jointly with a specialist ADHD or autism service, they can't prescribe or manage ADHD medication themselves. In practice, this can mean needing a referral to a separate ADHD screening or autism spectrum disorder assessment pathway alongside your perinatal mental health support, rather than one team handling everything. Worth asking your GP directly whether both referrals are needed, rather than assuming one covers the other.
Is it normal for perinatal anxiety to come out as anger or shutdown instead of worry?
Very much so, especially if you're neurodivergent. Anxiety is a state of overwhelm, and overwhelm can surface as irritability, anger, or a numb, shut-down, far-away feeling rather than classic worrying. You can read more about the anger side of this in RSD and Birth Trauma in ADHD and Autistic Mothers.
Will being autistic or ADHD affect my ability to look after my baby?
The honest answer is nuanced rather than simply reassuring, and I've set out the actual evidence on this further up rather than a soundbite version of it. In short: some studies find a slight link between certain autistic traits and self-reported bonding difficulty, while research observing real interactions between autistic mothers and their babies generally finds comparable warmth and responsiveness. Your anxiety is not a fair measure of your competence as a mother.
A gentle next step
If any of this rang true, you're not the only one who's felt it, and you don't have to work it out on your own. When you're ready, you're welcome to book a discovery call, where we can talk about what neuro-affirming support might look like for you.