
Birth Trauma Recovery: A Neuro-Affirming Map for Healing
By Tania Fragoso | Trauma-Informed & Neuro-Affirming Perinatal Counsellor
Most birth trauma content stays with the wound. This is about the path through it — what recovery actually looks like, why it isn't linear, and the part you play in it. Drawn from clinical practice, current research, and lived experience.
I met a woman the other day, and her daughter is about the same age as my twins. We were talking the way mothers talk when they think no one is really listening, which is to say: honestly.
As someone who has focused on birth trauma recovery, I have heard the version of this conversation many times before. Her daughter's birthday was coming up, and she said that every year, when that date came around, it brought with it the difficult feelings that she associated to her birth. Deep inside it had broken something in her. And the years since had been lived in the shadow of that breaking.
My own daughter had been with me that day. On the way home, she asked me quietly: Do you feel like that about us?
I thought about it properly before I answered. I said: it's not at all like that now. I can look back and feel a little sad. I think that feeling will always be there, and it makes sense.
I feel for the younger version of me who went through what I went through, and also for you and your sister, because I have seen how beautiful and gentle and even transcendental birth can be.
I often think about how different the world might look if more of us had that kind of entry into it. More healing, more peace, rather than the mess we so often start from.
But here is the thought that keeps coming back to me, after years of doing this work: I still don't know if people know that you don't have to live with your trauma. I still don't know if people know that it doesn't have to define you.
She said: OK, but it's hard, right?
Yes. It is hard, and really frightening, and not linear, and it might take a long time. But you can, one day, hold that part of yourself without it tearing you from the inside.
That is what this piece is about. Not the wound. It's about the non-linear path that healing can take, and the part we play in it.
Why recovery sometimes feels stuck, and why most of what you've read keeps you there
Most of the content available centres on the wound. There are awareness campaigns, accounts that catalogue what goes wrong, and communities where women gather around what happened and stay there. This serves a real purpose. Validation, witness, the profound relief of not being alone in something you could not previously say out loud. There is real value in this, and for many women, they are crucial. Being heard is where this work begins.
But being heard is not the same as healing. And the way we talk about trauma, collectively, matters more than we tend to acknowledge
Research on co-rumination, that is, the tendency to dwell on problems repetitively in peer conversations, even when those conversations feel supportive, shows that this kind of talk can deepen anxiety and depressive symptoms over time rather than relieving them (Tompkins et al., 2011). Support that circles the wound endlessly, without any movement toward integration, can keep a person stuck precisely because it feels like solidarity. It is difficult to leave a space where your pain is finally being witnessed. But witnessing is the beginning of the work, not the end of it.
Source: Tompkins, T. L., Hockett, A. R., Abraibesh, N., & Witt, J. L. (2011). A closer look at co-rumination: Gender, coping, peer functioning and internalizing/externalizing problems. Journal of Adolescence, 34(5), 801–811.

There is also something hard to mention, mostly because it can be perceived as assigning blame or invalidating the experience. And for someone who has just been through a birth experience that has left them deeply wounded, it can be very hard to conceive. It's like holding a single piece of a 100-piece puzzle without a guide, and trying to imagine what it looks like when it is all put together.
However, it deserves to be mentioned because it belongs in the space where recovery happens. The distinction between being a victim of something that genuinely happened to you, which is honest and accurate and the only valid starting point, and remaining in the victim position as an identity, which is where recovery quietly stops. The first is truth. The second is a pattern that many spaces unintentionally reinforce, not because anyone wants to harm, but because having both coexist in the same space would always harm the one that has just entered, and leave the ones that have successfully put their first pieces together, with no space for expansion.
You can talk about what happened. You cannot, in that same space, stop being the person it happened to.
What I hope to offer here is a bridge between the wound and the healing. What it actually looks like to move through it, not around it, and to come out on the other side as something other than defined by what happened.
What healing from a traumatic birth experience actually looks like — according to the women who have done it
Before looking at the clinical frameworks that support recovery, it is worth starting where we should always start: with the lived experience of the women who have actually moved through it.
A 2025 qualitative study using interpretive phenomenological analysis — a research approach that centres the detailed, subjective experience of participants — interviewed women who had experienced labour as a traumatic event and had moved through a process of recovery. Three things emerged consistently from what they described.
Healing is a process, not a destination. It is active and non-linear. It has milestones rather than a clear arrival point. Setbacks are not failure; they are part of it. The women in this study described being in a process that continued to unfold. The pieces arrive when ready to receive the next part of the puzzle.
Healing is being at peace with the experience, not free of it. The memory does not disappear. What changes is the relationship to it. It stops arriving uninvited, stops flooding the present, stops tearing you from the inside. You can hold it, look at it, speak about it, without the emotional charge taking over.
Healing is the capacity to hold multiple truths at once. You can grieve the birth you had and love the child who came from it. You can name the harm that was done and not be defined by it. You can be genuinely and permanently changed by it, and no longer be consumed by it.
These three findings are the frame that holds everything that follows. Every modality, every stage, every piece of clinical evidence cited in this piece is in service of exactly what survivors said healing is: a process, an integration, a capacity to hold complexity without being destroyed by it.
About the author: Tania Fragoso is a trauma-informed and neuro-affirming perinatal counsellor and coach, holding a Bachelor's in Mental Health Counselling from the Academie voor Coaching en Counselling in the Netherlands (2024). She is a certified doula (BIA Amsterdam, 2018) with seven years of birth support experience, a 3 Steps Rewind practitioner for birth trauma resolution (2022), and has trained in Anxiety in the Perinatal Period (TBR College of Perinatal Emotional Health, 2021), Supporting Survivors in the Perinatal Period (Resilient Birth, 2021), and Supporting Neurodiverse Birth (Neurodivergent Birth UK, 2024). She is an AuDHD mother of three, including twins, and works online with neurodivergent mothers internationally from her base in Málaga, Spain. Her approach is integrative, trauma-informed, and explicitly neuro-affirming.
An integrated, neuro-affirming map of birth trauma recovery
Recovery is not based on a single approach, and not all approaches will suit everyone. It is a structured progression in stages that build on each other. What follows is the framework that underpins the work I do with clients, drawn from clinical evidence.
It comes from the theorists and practitioners who developed the modalities that make up this approach, and from the lived experience of the women I have sat with over seven years of perinatal work, and my own recovery.
Read it as a map, not a prescription. Not everyone moves through every stage at the same pace, or in exactly the same order. The work is rarely tidy. But the shape of it, broadly, is this.
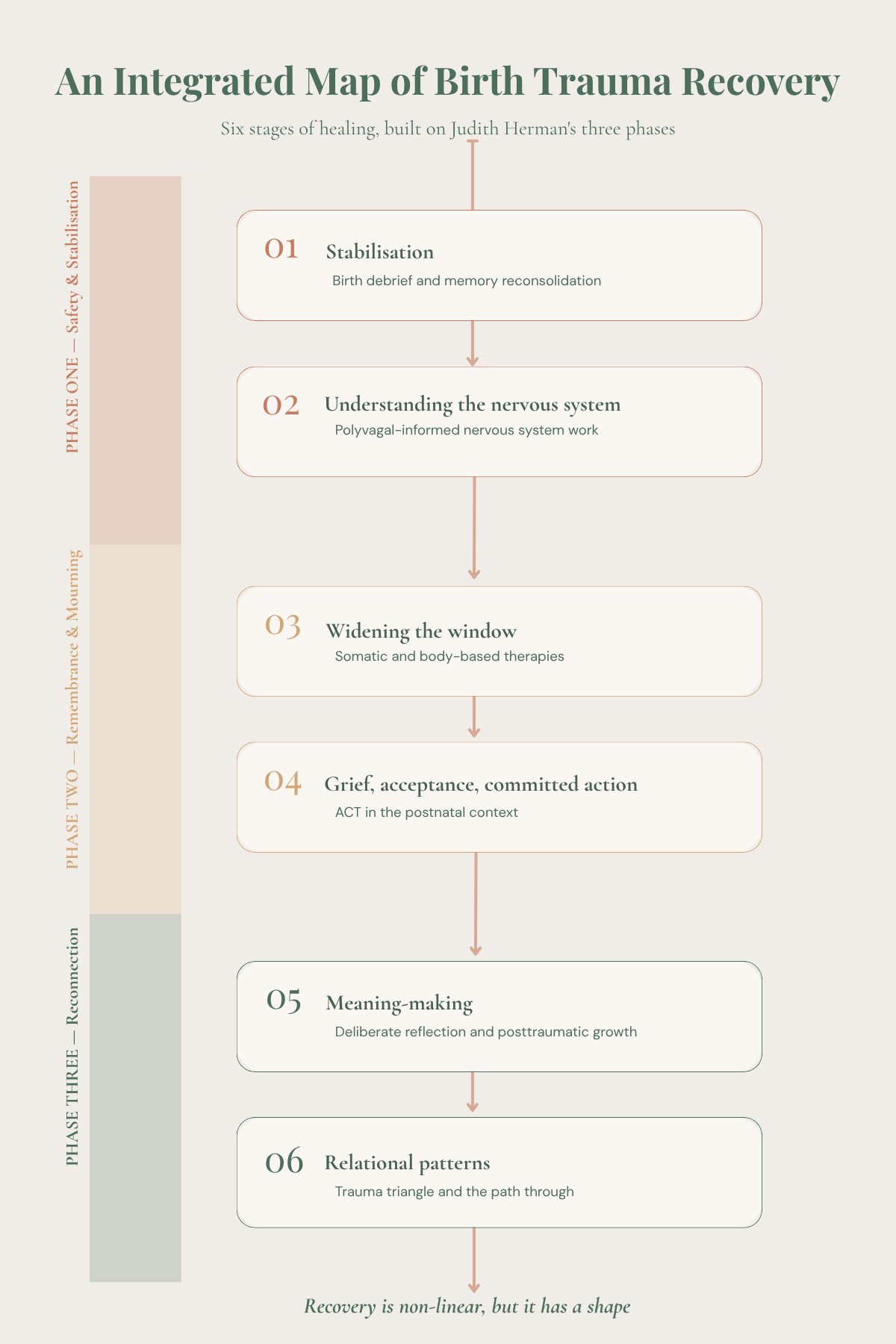
The six stages of recovery, mapped onto Judith Herman's three-phase framework. Recovery is non-linear, but it has a shape.
Stage 1: Stabilisation — birth debrief and mental health support
This part is often skipped. Women often seek help at a point where they are truly struggling and exhibiting signs that point to postnatal depression, so they start addressing the symptoms that relate to the diagnosis and jump over the wound that got them there. In the meantime, they might be experiencing symptoms of PTSD, and their nervous system is continuously flooded and unable to discern what might have been the root cause of it.
A Birth debrief, or birth afterthoughts, offers an opportunity for stabilisation. It's a structured, trained, empathic dialogue led by a specialised midwife or healthcare provider that helps a woman reconstruct the timeline of her birth, understand what happened and why, name what she felt, and begin to place the experience rather than have it continue to arrive when you least expect it.
What a birth debrief covers:
Reconstructing the timeline of what happened
Understanding what was clinical and what was not
Naming what you felt at each point
Placing the experience so it stops arriving uninvited
A review of this kind of approach has been associated with meaningful symptom reduction and high participant satisfaction (Thomson & Nowland, 2024). A 2024 systematic review and meta-analysis of 41 trials found that both trauma-focused therapies and dialogue-based counselling interventions delivered after a difficult birth experience produced moderate-to-large reductions in Post-Traumatic Stress Disorder symptoms (Dekel et al., 2024).
Sources: Thomson, G., & Nowland, R. (2024). Postnatal listening services for women after traumatic birth: A rapid review. Midwifery, 132, 103972. Dekel, S., Papadakis, J. E., Quagliarini, B., Pham, C. T., Pacheco-Barrios, K., Hughes, F., Jagodnik, K. M., & Nandru, R. (2024). Preventing posttraumatic stress disorder following childbirth: A systematic review and meta-analysis. American Journal of Obstetrics and Gynecology, 230(6), 610–641.e14.

sits at this stage. It is a structured memory reconsolidation approach that focuses on working with the way difficult or traumatic memories are encoded and retrieved, to reduce the emotional charge attached to the memory without erasing or distorting its content. It is used in clinical perinatal practice and is part of the integrative toolkit described in this piece.
The aim of stabilisation is not to resolve the trauma. It is to make the rest of the recovery journey possible.
Stage 2: Understanding the nervous system — effects of birth trauma on the body's threat response
The effects of birth trauma are not only in the memory. They change how your nervous system reads the world around you, and more specifically, whether it reads it as safe.
It helps to clear up something first, because it gets muddled often. Trauma is not simply "in your head," something to be reasoned away with the right thought or the right reframe. But it is not simply "in your body" either, waiting to be released like a held breath. It is held in the whole system: brain and body working as one continuous loop, each constantly speaking to the other. This is why the old idea of treating the mind and the body as separate things gets recovery wrong. You cannot think your way out of something your body is still bracing against, and you cannot soothe your body while your mind is still convinced it is in danger. The two are not separate. They never were.
A consensus has been building for decades across the trauma-focused therapies — through Pat Ogden's Sensorimotor Psychotherapy, Janina Fisher's work with the traumatised parts of the self, Peter Levine's Somatic Experiencing, and more recently Arielle Schwartz's integration of these approaches with posttraumatic growth research. What they share is the understanding that recovery has to reach both the story and the system that holds it. Approaches that work only with the narrative, like talking therapies, frequently fail to reach what the nervous system is still carrying (Ogden, Pain & Fisher, 2006).
One of the most widely used frameworks for explaining this is Stephen Porges's Polyvagal Theory.
It describes how the nervous system moves between states of safety and connection, mobilisation (fight or flight), and shutdown (collapse, dissociation, numbness). It has been hugely influential in how trauma is understood, and it remains a useful way of making sense of what survivors actually experience, even as some of its finer scientific claims continue to be debated. You do not need the theory to be settled to recognise yourself in it.
What is not in dispute, and what you will likely know in your own body if you have lived through a traumatic birth, is this: the nervous system does not simply go back to how it was before once the event is over. Dan Siegel's idea of the window of tolerance names it well. There is a zone within which you can think, feel, connect, and cope. Inside the window, you are present. Outside it — flooded by too much, or shut down into too little — the parts of you that can reflect, relate, and make sense of things cannot come online. Trauma narrows that window. Things that would not have rattled you before now tip you over the edge, or drop you through the floor. Prentis Hemphill describes the work of widening it again as building the capacity to stay with what is — not running from what is hard, nor drowning in it.
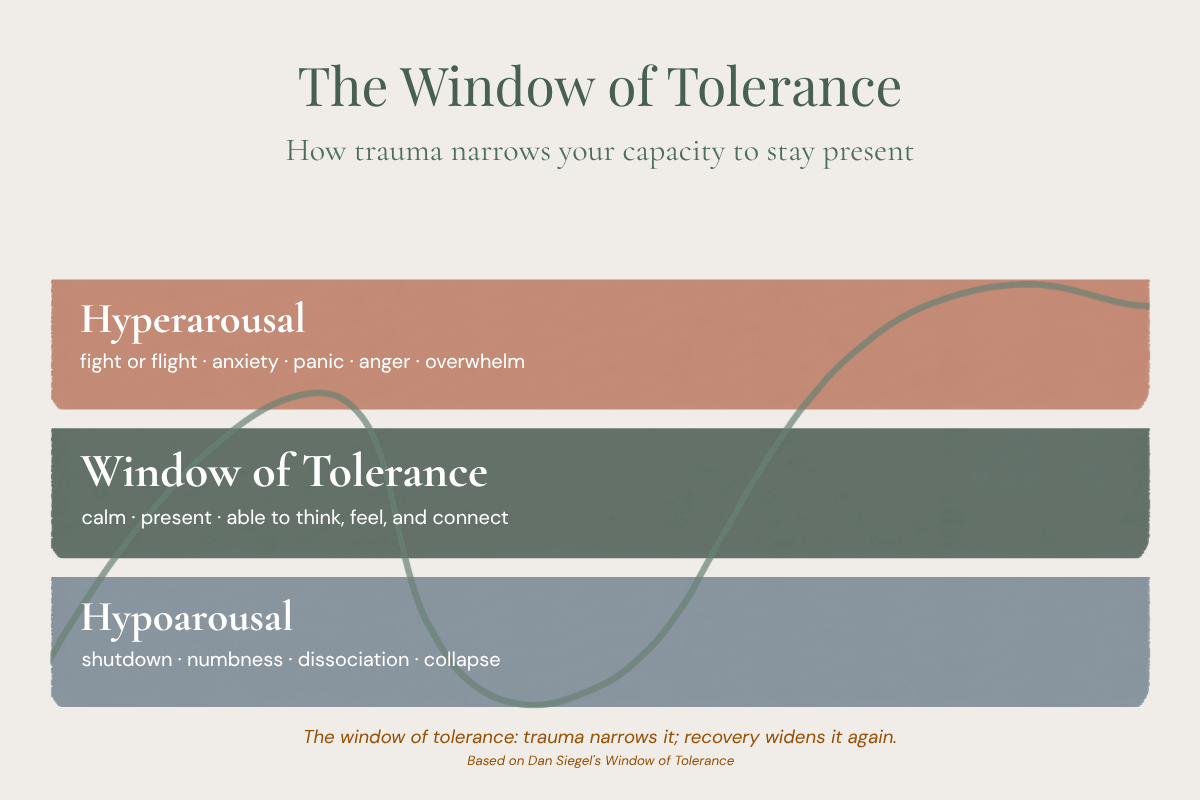
The window of tolerance: trauma narrows it; recovery widens it again.
Underneath all of this sits Judith Herman's stage model of trauma recovery, first described in Trauma and Recovery (1992) and still the framework most widely used today: safety and stabilisation, then remembrance and mourning, then reconnection. The map you are reading is built on this architecture, with each stage named for the work it contains. Recent research continues to show that building stability first, before moving into the harder work of processing, leads to better outcomes, especially when the wound is deep or layered (Melegkovits et al., 2022).
Source: Melegkovits, E., Blumberg, J., Dixon, E., Ehntholt, K., Gillard, J., Kayal, H., Kruczkowska, S., Pelidou, M., Spens, A., Walsh, E., Billings, J., Robertson, M., & Bloomfield, M. (2022). The effectiveness of trauma-focused psychotherapy for complex post-traumatic stress disorder: A retrospective study. European Psychiatry, 66(1), e4
This is not background theory. It is the ground everything else stands on. And it is why working with the body is not an add-on to recovery, it is at the centre of it.
Stage 3: Widening the window — somatic and body-based work
The importance of the body in the recovery path is essential. This is where somatic approaches earn their place, as primary therapeutic modalities with robust evidence.
Somatic Experiencing, developed by Peter Levine, works with the body's interrupted survival responses — the impulses toward fight, flight, and freeze that were activated during the traumatic birth and never had the opportunity to complete. Through titration (approaching difficult material in very small doses) and pendulation (moving between distress and relative ease), somatic work gradually helps the body discharge what it has been holding and rebuild a felt sense of safety. A randomised controlled trial of Somatic Experiencing for PTSD found large, sustained reductions in PTSD symptoms (Cohen's d 0.94–1.26) and depression (d 0.7–1.08) at follow-up (Brom et al., 2017).
Source: Brom, D., Stokar, Y., Lawi, C., Nuriel-Porat, V., Ziv, Y., Lerner, K., & Ross, G. (2017). Somatic experiencing for posttraumatic stress disorder: A randomized controlled outcome study. Journal of Traumatic Stress, 30(3), 304–312.
For birth trauma specifically, body-based work matters in a way that is particular and often unspoken: the trauma happened in the body. Touch, intervention, loss of control over what was being done to you, the positions you were placed in, the sensations of pain or numbness or disconnection — these are not abstract memories stored only in narrative. They live in tissue, in posture, in the way you hold your breath in clinical settings, in the visceral response that arrives before you have any conscious thought. Somatic work gives the body a way to process what the mind cannot always reach, and to begin rebuilding what the birth disrupted: the basic sense that your body is a safe place to inhabit.
Stage 4: Grief, acceptance, and committed action — ACT in the postnatal context
A traumatic experience is rarely only what happened. It is also the loss of what was meant to happen. The birth imagined, prepared for, hoped for. The welcome your baby deserved and did not receive. The version of yourself you thought would be there to bond with your baby, and wasn't, because you were too frightened, too alone, too shocked, or too busy surviving.
Recovery has to make space for that grief. It cannot be bypassed.
Acceptance and Commitment Therapy (ACT), developed by Steven Hayes, is one of the most useful frameworks for this stage. It does not ask you to feel differently about what happened. It does not ask you to reframe the trauma or find the silver lining. It asks you to make room for what you actually feel. All of it. This includes the grief, the anger, the fear, the regret, to be able to co-exist in the presence of those feelings rather than despite them, and move toward what you genuinely value.
ACT has been identified as particularly well-suited to perinatal populations precisely because it addresses values, acceptance, and the additional burden of stigma that mental illness in this period carries (Bonacquisti et al., 2017). Another study focused on the applicability of ACT in this period found that aceptance focused process and self-compassion protected at-risk postpartum women from developing depressive and anxiety symptoms..
Sources: Bonacquisti, A., Cohen, M. J., & Schiller, C. E. (2017). Acceptance and commitment therapy for perinatal mood and anxiety disorders: Development of an inpatient group intervention. Archives of Women's Mental Health, 20(5), 645–654. Monteiro, F., Fonseca, A., Pereira, M., & Canavarro, M. C. (2022). The role of acceptance-focused processes and self-compassion. Journal of Affective Disorders, 308, 268–276
ACT lets you carry the grief alongside the life you are living and building, rather than waiting for the grief to be finished before you can be present. For many mothers, this makes all the difference.
Stage 5: Meaning-making — deliberate reflection and posttraumatic growth
Posttraumatic growth is real. It is documented. And it is widely misunderstood.
It's a concept developed by Richard Tedeschi and Lawrence Calhoun — refers to the positive psychological change that can emerge from the struggle with highly challenging life events. It is not the silver lining. It is not the suggestion that your trauma was secretly a gift. It is the recognition that some people who have moved through something genuinely devastating emerge with a changed relationship to their own life: a different sense of what matters, a deepened connection with others who have struggled, a changed understanding of their own capacity.
Research in the birth trauma context shows that posttraumatic growth after childbirth is real but dependent on individual factors, the nature of the experience, and, most importantly, contextual support (Brandão et al., 2020).
A 2024 study identified the mechanism that drives posttraumatic growth: Deliberate rumination, as opposed to intrusive rumination. This means that focusing and reflecting intentionally and making some meaning out of it, rather than the rumination that is involuntary and looping, which is a symptom of traumatic stress itself. (Brandão et al., 2024).
Sources: Brandão, T., Brites, R., Hipólito, J., Pires, M., & Nunes, O. (2020). Posttraumatic growth after childbirth in women with postpartum depression: A descriptive cross-sectional study. Journal of Clinical Psychology in Medical Settings, 27(4), 685–692. Brandão, T., Brites, R., Pires, M., Hipólito, J., & Nunes, O. (2024). Rumination, posttraumatic stress, and posttraumatic growth following childbirth: A path analysis approach. Psychological Trauma: Theory, Research, Practice, and Policy. Advance online publication.
One is integration work, and the other is what you're doing before the work begins.
Stage 6: Relational patterns — the roles trauma pulls us into
This is also where positive psychology earns a careful place. Martin Seligman's PERMA model — Positive emotion, Engagement, Relationships, Meaning, Accomplishment — is not a prompt to look on the bright side. It is a framework for identifying what makes a life feel worth the work of recovering. People do not heal from trauma because they are told to be grateful. They heal because they find something strong enough to want to be different on the other side of it. And in my own experience, and in the work I do with mothers, that something is so often their children, the source of the meaning and motivation that makes a woman willing to begin the work of recovery in the first place.
Every recovery happens inside relationships: with a friend or family member, a healthcare system, and very often a community of other people who have been through something similar. The patterns that form in those relationships matter as much as the individual work, and this is the stage that tends to receive the least attention.
There is a well-known framework from Transactional Analysis, developed by Eric Berne, that helps make sense of these patterns. Stephen Karpman's drama triangle describes three roles people move between under stress: Victim, Rescuer, and Persecutor. More recently, clinicians have begun to build on this and call this the trauma triangle, because after such an event, these are not simply unhelpful habits; they are survival states.
the three roles of the trauma triangle:
Victim — seeks protection and safety after harm
Rescuer — seeks worth and connection through caring for others
Persecutor — seeks power and control after a period of having none
Each one is an attempt to stay safe: the Victim seeks protection, the Rescuer seeks connection and worth through caring, the Persecutor seeks power and control after a period of having none. Trauma-informed care understands these responses as exactly that, adaptive attempts to cope, not flaws to be ashamed of (SAMHSA, 2014).
Source: Substance Abuse and Mental Health Services Administration (2014). Trauma-Informed Care in Behavioral Health Services. Treatment Improvement Protocol No. 57. U.S. Department of Health and Human Services. Read the protocol
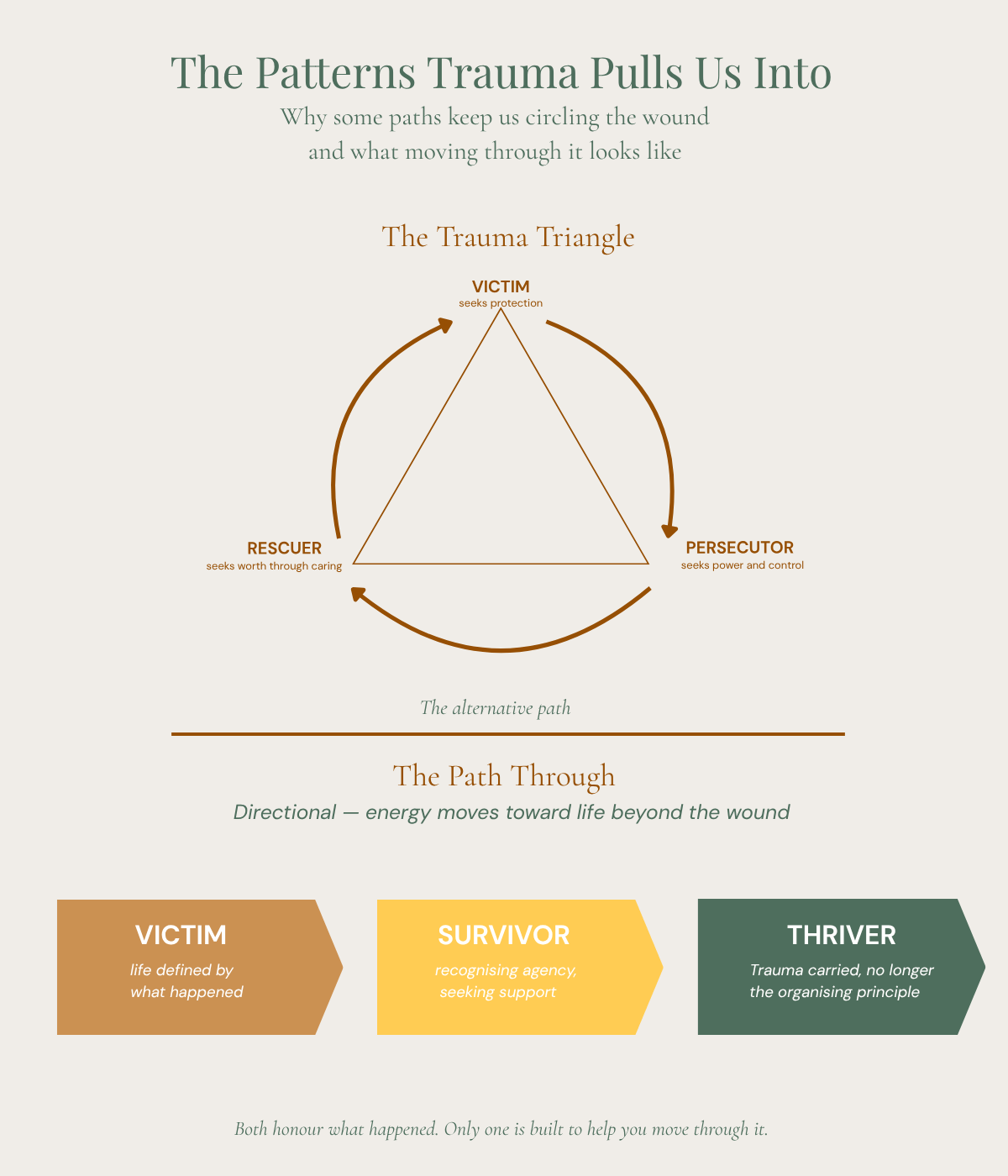
The trauma triangle keeps the roles circling. The Victim-Survivor-Thriver path moves forward — same wound, different direction.
After a difficult or traumatic birth, the Victim position is not just understandable; in the sense that something genuinely happened to you, it is accurate. The difficulty is when it quietly becomes an identity rather than a starting point, when life reorganises itself around the wound and stays there. The Rescuer is often a partner, a friend, a fellow survivor, or a professional, doing the essential work of holding someone in their pain, but sometimes at the cost of their own boundaries and regulation.
The Persecutor can be the system that failed you, the people who did not protect you, and sometimes, painfully, yourself.
I can speak to this honestly because I lived it. When I became a doula, I wanted to be a saviour. I remember writing my business plan and putting down, as my ethos, that I wanted to save women from ever experiencing the same trauma I had, and while doing it, tears fell freely down my face. What I understand now is that the wound was still wide open. Clinically, I was no longer suffering from PTSD, depression, or anxiety. By every diagnostic measure, I had recovered. But my nervous system still had no safety in it whenever I spoke about my own birth, six years on. I had become symptom-free without ever having healed.
That distinction is one of the most important things I have learned, in my own life and in my work:
being symptom-free is not the same as being healed.
You can meet none of the diagnostic criteria and still be organised entirely around an unhealed wound. Recovery is not the absence of difficult responses; it is a changed relationship to them (SAMHSA, 2014).
This is also why the spaces we recover in matter so much. A community can hold the birth stories and its wound in place, or it can support movement through it. The trauma triangle is circular, meaning that the roles swap, the energy keeps orbiting the original injury, and everything stays in motion without going anywhere. The alternative is a different and more hopeful path, widely described in trauma work as the movement from Victim to Survivor to Thriver. The Victim's life is defined by what happened. The Survivor begins to recognise their own agency, seeks support, and experiments with boundaries. The Thriver carries the trauma as part of their story without it being the organising principle of their life; instead, identity reorganises around meaning, values, and what comes next.
The difference between the two is direction. One is circular and keeps energy bound to the wound. The other is developmental, and slowly turns the energy toward life after trauma. Wound-centred communities, even the most well-meaning ones, can quietly stabilise the Victim position, because that is what holds the community together. Recovery-oriented spaces welcome the wound, but organise around safety, skills, nervous-system literacy, connection, and forward motion. Both validate what happened. Only one is built to help you leave.
Birth trauma years later — why time alone doesn't heal it
One of the quietest griefs is the discovery that time, on its own, does not resolve it. Years pass. The baby grows. The story gets told differently, or stops being told at all. You think you have moved on. And then a birthday comes around, or a particular smell, or a hospital corridor, or a friend announces a pregnancy, and you are suddenly back inside it, feeling the pain and sorrow as sharply as if no time had passed at all.
This is not a sign that you have failed at recovering. It is a sign that your relationship to the original wound hasn't yet been addressed.
Trauma is stored not only as narrative memory but also as implicit and somatic memory. Held at a nervous system level, in the responses that activate before the conscious mind has caught up. This is why anniversary reactions are not irrational; they are the body recognising something it encoded at a level deeper than story.
Implicit memory does not soften with time. It softens with the right kind of contact: with a mental health professional who can hold the story without being overwhelmed by it, with approaches that work at the level of the body and the nervous system, with the slow work of processing that the ordinary passage of days and years cannot substitute for.
I see this most clearly in the women who come to me during a second pregnancy. They had not addressed the pain of the first birth. Life moved on, the baby grew, there was no time and perhaps no language for it, and now, with the approaching birth of another baby, it has brought all of it to the surface. For some, the first Braxton Hicks contraction is enough. That single physical sensation sends them straight back into the original moment, as though it were happening again, as though no years had passed at all. The body recognised the cue before the mind had any say in it.
It is also something I hold carefully with survivors of sexual abuse, for whom the vulnerability that birthing asks for can reactivate a much older wound, through loss of control, exposure, and things being done to the body. Birth does not always create trauma from nothing. Sometimes it presses on what was already there.
If your experienced birth trauma five years ago, or ten, or more and if you are reading this because a date is coming and you still don't quite know how you will get through it, this piece is for you as much as for the woman who gave birth last month. The research on posttraumatic growth details that healing does not have a window. It has the willingness and the right conditions. Both of those can be created at any point.
You are not too late.
What active participation in your own healing means
There is something I have been thinking about for a long time, and that I want to say as clearly as I can, because I don't think it gets said enough.
You don't have to live with your trauma. It does not have to define you.
Those sentences sound simple. They are not. Because the next question — the one your daughter or your partner or some quiet part of yourself will ask — is: but it's hard, right?
Yes. It is hard. It is frightening. It is not linear, and it may take longer than you want it to. There will be sessions that feel like nothing happened, and weeks where it seems to move backwards, and moments where you wonder whether this is just what your life is now. That is all part of it.
What I have found from both my own recovery and in sitting with clients over many years is that the hardest part of healing is not the therapeutic work itself. The hardest part is the shift from being someone this happened to into being someone actively engaged in what happens next. From I am the person who had that birth to I am the person in the process of integrating that birth. It is a subtle distinction that changes everything about how you relate to the work.
Active participation does not mean you are responsible for the wound. Nothing about what happened to you at birth was your fault. It does not mean you should have started sooner. It does not mean you are failing when it is slow.
It means: the wound is real, and the work of integrating it is yours. No one can do it for you. No number of hours spent in online communities talking about it will do it for you. You have to be willing to look at the whole, the life before the birth, the person you were when you walked in, the events of the birth itself, and the years since. To grieve what you lost. To understand what made you more vulnerable. To feel what you have been managing not to feel. To ask uncomfortable questions and sit with the answers.
And to know — because this is what the women on the other side of it will tell you — that one day, you can hold that part of yourself without it tearing you from the inside.
A note for neurodivergent mothers
The map described in this piece needs adapting for neurodivergent mothers — those of us who are autistic, ADHD, or AuDHD — because every stage of the recovery process is shaped by how our brains and nervous systems work. A few things matter particularly:
Interoception. Many autistic and ADHD people have a different, often reduced or unreliable, relationship to internal body signals. Somatic work may need to be adapted, more cognitively framed, and taken more slowly. Standard instructions can land as deeply confusing rather than grounding. I have created a free resource that can help reconnect to these signals; you can download it here.
Alexithymia. Difficulty identifying and naming emotional states is common in autistic people and in those with ADHD burnout. Postnatal mental health: therapeutic approaches that rely on emotional labelling as a primary tool can increase difficult feelings rather than reduce it. Recovery work that is adapted for alexithymia looks different and moves at a different pace.
Masking and autistic burnout. If you spent your pregnancy and birth in a state of sustained masking — performing the version of yourself that clinicians and birth professionals expected, suppressing your actual needs and responses to be compliant, this creates an extra layer of depletion that most non-neurodivergent practitioners won't see. Recovery has to acknowledge this. You can take the free assessment here.
Rejection sensitive dysphoria. Birth trauma in an RSD-prone nervous system often carries an additional and specific layer of shame: the sense that you should have done better, that you failed somehow, that your responses in the room were wrong. The replaying is not only of what happened, but of what you did or didn't do. This needs a particular kind of attention, one that understands RSD and doesn't inadvertently reinforce the shame. I have created a resource to get you started; you can access it here.
Executive function. Recovery requires consistent showing up: sessions, practices between sessions, the work of integration across ordinary life. For ADHD mothers, the executive function load of doing the work is itself part of the challenge, and it needs scaffolding. Not more willpower. Practical structure.
A neuro-affirming approach to post-birth trauma healing does not mean a fundamentally different map. It means a map whose practitioner knows how to read the terrain for brains that work the way yours do.
You can hold it without it tearing you from the inside — closing thoughts
The mother I met, the one whose daughter's birthday brings everything back, every year, is not unusual. She is one of the many. Women who loved their babies and grieve the birth they had. Women who have spent years wondering whether this is simply what it is to have had that experience. Women who did not know, and still don't know, that there is work that can reach this, and that it doesn't have to stay like this.
I said, on the walk home: it is hard. It is frightening. It is not linear, and it takes as long as it takes. But one day, with the right support, the right work, the willingness to look at the whole of it, you can hold that part of yourself without it tearing you from the inside.
That is not a promise of resolution. It is not the suggestion that the birth will stop mattering, or that you will be grateful for it, or that you will reach some state of complete peace that means nothing can ever touch it again. It is something more modest and more true: the possibility of a different relationship to what happened. Integration rather than fragmentation. Being the person who carries this, rather than the person being carried away by it.
If you are still carrying a birth that happened years ago, if a date approaches and you do not quite know how you will get through it, I want you to know that what you are carrying is real, and that there is work that can meet you where you are.
You do not have to start this work alone.
If you are ready to begin, you can find out more about how we can work together so you can have the support you need, or download the Postpartum Survival Guide as a starting point. Both are here for you, wherever you are in the journey.
Frequently Asked Questions
If you are ready to begin, you can find out more about how we can work together so you can have the support you need, or download the Postpartum Survival Guide as a starting point. Both are here for you, wherever you are in the journey.
-
It is shaped less by what happened on paper and more by how their experience of birth was perceived. Two women can have the same obstetric event — an emergency caesarean, an instrumental delivery, postpartum haemorrhage or vaginal birth that led to birth injuries — and one walks away shaken but intact, while the other is left with trauma. What tends to make a birth traumatic is the felt sense of it: losing control, not being listened to, feeling unsafe or unseen, having things done to your body without consent or explanation, fearing for your life or your baby's. Care that is rushed, dismissive, or frightening can be as wounding as any medical complication. And for some women, birth presses on an older wound — a previous trauma, including sexual trauma — that was already there. The event matters, but it is your experience of it that determines the imprint it leaves.
-
There is no single timeline, and anyone who gives you one is likely oversimplifying.
Brief structured treatment options delivered after a traumatic birth can produce meaningful symptom reduction within weeks (Dekel et al., 2024).
Deeper integration work, such as building nervous system capacity, processing grief, and finding meaning, typically unfolds over months to years, and it is non-linear. What matters far more than speed is to find support that suits your unique needs, at the right stage of the work. The research is clear: healing is a process. Starting that process, at any point, matters more than how quickly you move through it.
-
The memory does not disappear, and it is not the goal of recovery to make it disappear. What changes, through the work, is your relationship to the memory. Women and birthing people who have moved through birth trauma describe healing as being able to hold the impact of the birth — to speak about it, to remember it, to be reminded of it — without being overwhelmed or undone by it. This is integration, not erasure. The birth happened. Recovery is not about making it un-happen. It is about no longer being ruled by it.
-
Yes. Trauma is stored not only as narrative memory but as somatic and implicit memory — held in the autonomic nervous system, in muscle tension, in posture, in the automatic responses that activate in response to specific triggers: a particular smell, a medical environment, a position, a date on the calendar. This is why talking alone rarely resolves it completely. Polyvagal-informed and somatic approaches work directly with this body-held memory, which is why they form a central part of an integrated recovery approach.
-
Yes — often years later, and sometimes decades later. It can shape subsequent pregnancies and births, parenting confidence, relationships, sexual intimacy, body image, and the broader sense of self. It can resurface at anniversaries, at developmental milestones of a child, at moments that echo the original experience. Late-emerging or intensifying symptoms are not a sign that you have made things worse by waiting. They are a sign that the work of integration hasn't yet happened, and that your nervous system is still carrying feelings about your birth.
-
It varies, but common experiences include: intrusive memories or images of the birth that arrive without being sought, flashbacks that feel as immediate as the original event, hyperarousal (being easily startled, vigilant, unable to rest) or numbness and disconnection, avoidance of anything that triggers the memory, difficulty bonding with a baby or older child, disturbed sleep, and a sense that the person who walked into that birth did not walk out — that something essential was lost in that room and has never quite been retrieved. None of these responses are signs of weakness or of being unable to cope. They are signs of an event that has not yet been integrated.
-
The most important first step is being heard properly — not by someone who will reassure you and move on, but by a practitioner trained in birth trauma who can hold the full weight of the story, help you reconstruct and understand what happened, and begin the work of placing it rather than being placed by it. A structured birth reflection or a memory reconsolidation technique, such as the 3 Steps Rewind can reduce the emotional charge of the memory enough to make the deeper work possible. From there, the path unfolds through nervous system understanding, somatic work, grief and acceptance, meaning-making, and the relational work of moving out of the patterns trauma pulls you into. If you are not sure where you are on this map, reach out to your GP or health visitor as a first step and discuss treatment options. Whatever path you take, the most important thing is to get the support that you need. Find out more about Neuro-Affirming Birth Debrief
-
The 3-3-3 rule is a simple grounding technique often shared with new mothers who are experiencing anxiety, intrusive thoughts, panic, or flashbacks — common after a traumatic birth. It works by drawing your attention back into the present moment through your senses. Look around you and name three things you can see. Pause and notice three sounds you can hear. Then move three parts of your body — wiggle your fingers, roll your shoulders, press your feet into the floor.
It can be a genuinely helpful tool in the moment, especially when distress comes on quickly and you need something to bring you back. But it's worth being honest about what it does and doesn't do. Grounding techniques settle the immediate wave of activation. They do not heal what's underneath it. If you find yourself reaching for them often — if grounding has become how you get through the days rather than a tool for occasional moments — that is a sign that the wound underneath is asking to be addressed properly. There is more support available than this.